What Are the Most Common Rapamycin Side Effects — and How Do You Actually Manage Them?

Rapamycin is currently the most effective known pharmaceutical for extending lifespan and delaying age-related diseases in mammals. While its potential to enhance human healthspan is supported by a growing body of evidence, many users are deterred by fears of adverse events like mouth sores, metabolic shifts, and immune suppression [1] [2]. This authoritative guide breaks down exactly how to identify, manage, and prevent these side effects based on current clinical data and expert protocols.
Why Does Rapamycin Cause Mouth Sores, and How Common Is It at Longevity Doses?
Mouth sores are the most frequently reported side effect of rapamycin, appearing in roughly 15% of longevity users compared to over 70% of oncology patients [3]. They are typically transient, benign, and manageable with topical steroids [4]. Understanding the distinct mechanism of these ulcers allows for effective treatment without necessarily discontinuing the drug [3] [5].
What Is mTOR Inhibitor-Associated Stomatitis (mIAS), and Is It the Same as a Regular Canker Sore?
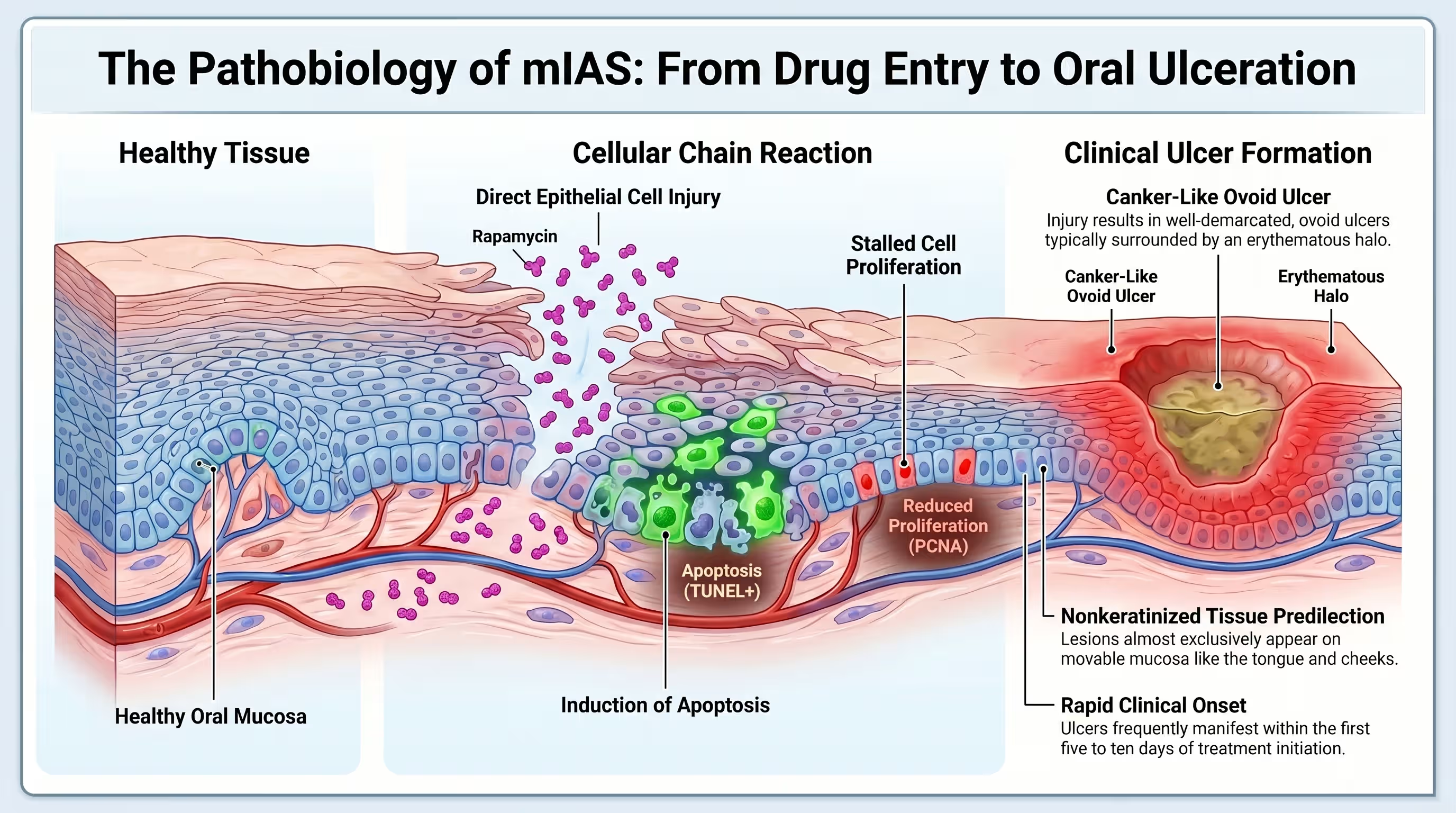
mTOR inhibitor-associated stomatitis (mIAS) refers to discrete, painful ulcers that clinically resemble recurrent aphthous stomatitis, or “canker sores”. Unlike conventional chemotherapy-induced mucositis, which causes widespread tissue sloughing, mIAS presents as small, ovoid ulcers with an erythematous halo. These lesions are localized to the movable mucosa, such as the lips and tongue [5] [6] [7].
Clinicians originally mislabeled mIAS as “mucositis,” assuming it shared the same pathobiology as cytotoxic chemotherapy side effects. However, research characterizes mIAS as a distinct clinical entity. While chemotherapy causes direct DNA damage and global tissue destruction, rapamycin inhibits the mTORC1 and mTORC2 complexes, which regulates cell proliferation and survival [5] [6] [7].
The initiation of mIAS is likely driven by direct epithelial cell injury. Specifically, rapamycin reduces cell nuclear antigen (PCNA) and increases markers of apoptosis (programmed cell death) even at low concentrations. This process is independent of the oral microbiome, meaning bacteria are not the primary cause [3] [6].

How Soon After Starting Rapamycin Do Mouth Sores Typically Appear?
Mouth sores typically emerge very quickly after starting therapy, often within the first cycle of treatment or even within the first five days of administration. Most cases in longevity cohorts are reported within the first few months. Early detection and proactive topical management are key to preventing these lesions from interfering with dosing schedules [5] [6].
In clinical trials, the median time to onset of oral ulceration was approximately 10 days for cancer patients and roughly 55 days for stem cell transplant recipients [4] [6]. For those taking rapamycin off-label for healthspan, intermittent ulcers are frequently reported as disappearing even with continued usage [8].
This rapid onset suggests a swift biological effect on the renewing cells of the oral mucosa. Paradoxically, some evidence indicates that the incidence of mIAS may actually decrease during subsequent courses of treatment, a phenomenon that contradicts the cumulative toxicity patterns seen with traditional chemotherapy [6].
Which Dose and Dosing Frequency (Daily vs. Weekly) Carries the Highest Risk of Mouth Sores?
Higher doses and daily administration frequencies significantly increase the risk and severity of stomatitis. In renal transplant studies, incidence rose from 10% in patients taking 2 mg daily to 20% in those taking 5 mg daily [4] [6]. Longevity protocols often utilize once-weekly dosing to reduce these trough concentrations and minimize oral side effects [8] [9].
The relationship between rapamycin concentration and mIAS is well-documented [6]. Daily dosing regimens maintain high “trough” levels of the drug in the blood, which continuously suppresses mTOR signaling in mucosal tissues [9]. In contrast, weekly or bi-weekly “pulsatile” dosing allows for a high peak concentration followed by a drug-free period, which may allow for tissue recovery [10] [11].
Interestingly, survey data of off-label users found that those reporting persistent ulcers were actually taking lower average doses (3.6 mg/week) than those reporting intermittent ulcers (6.87 mg/week). This suggests that individual sensitivity and genomics may play a larger role in risk than dose alone for the longevity population [6] [8].

What Are the Most Effective Treatments for Rapamycin-Related Mouth Sores — Rinses, Topicals, or Dose Reduction?
Topical corticosteroids are the gold-standard treatment, providing symptom relief and faster resolution in over 87% of cases [3] [4]. Specifically, a dexamethasone mouthwash is recommended as a therapeutic intervention rather than a preventative measure [3] [6]. Dose reduction or temporary drug holidays are effective secondary strategies if sores become severe or interfere with eating [5].
Because mIAS involves a localized inflammatory response, anti-inflammatory medications are highly effective. While rapamycin itself is immunosuppressive, steroids manage the sores through a distinct non-immunologic mechanism by modulating the mTOR pathway to interfere with proinflammatory cytokine release [6].
Other palliative treatments include:
- Magic Mouthwash: Often contains lidocaine and aluminum/magnesium hydroxide for pain management [4].
- Clobetasol Gel (0.05%): Applied directly to ulcers via a gauze pad for 5-10 minutes twice daily [5].
- Low-Level Laser Therapy (LLLT): Emerging as a potential treatment to decrease inflammatory cytokine expression, though clinical validation for mIAS is still ongoing [3].
Does Steroid Mouthwash (Dexamethasone Rinse) Actually Resolve mIAS Faster?
Yes, clinical trials like the SWISH study proved that dexamethasone mouthwash reduces the incidence of grade 2 or higher mucositis by over 90%. Users swish 10 mL of solution (0.5 mg/5 mL) for two minutes, four times a day. This protocol allows patients to continue their primary treatment without dose modifications [3].
Can Vitamin C, Zinc, or Omega-3 Supplements Reduce the Frequency of Mouth Ulcers?
While clinical trials for these specific supplements in mIAS are sparse, maintaining optimal nutritional status is a recognized factor in oral health. High-dose Vitamin C and Zinc are often utilized in general “biohacking” protocols to support tissue repair, but they are considered secondary to established topical steroid interventions for mIAS [5] [12].

When Should Persistent Mouth Sores Prompt a Dose Reduction or a Pause in Rapamycin?
If mouth sores become symptomatic enough to limit a normal diet or if “patchy” ulcerations appear, users should temporarily pause the drug. Dosing can typically be re-initiated once the sores resolve to grade 1 (mild erythema or soreness). Persistent, high-grade pain that prevents liquid intake (grade 3) requires a permanent dose reduction [3] [5].
How Does Rapamycin Affect Your Cholesterol and Triglycerides — and What Can You Do About It?
Hyperlipidemia is a hallmark side effect, with sirolimus often causing a dose-dependent increase in triglycerides and LDL cholesterol. In transplant patients, total cholesterol has been shown to increase by an average of 50%. Fortunately, these metabolic shifts are reversible within 1-2 months after stopping the drug and can be managed through diet or supplementation [13] [14].
Why Does Rapamycin Raise Triglycerides and LDL Cholesterol in the First Place?
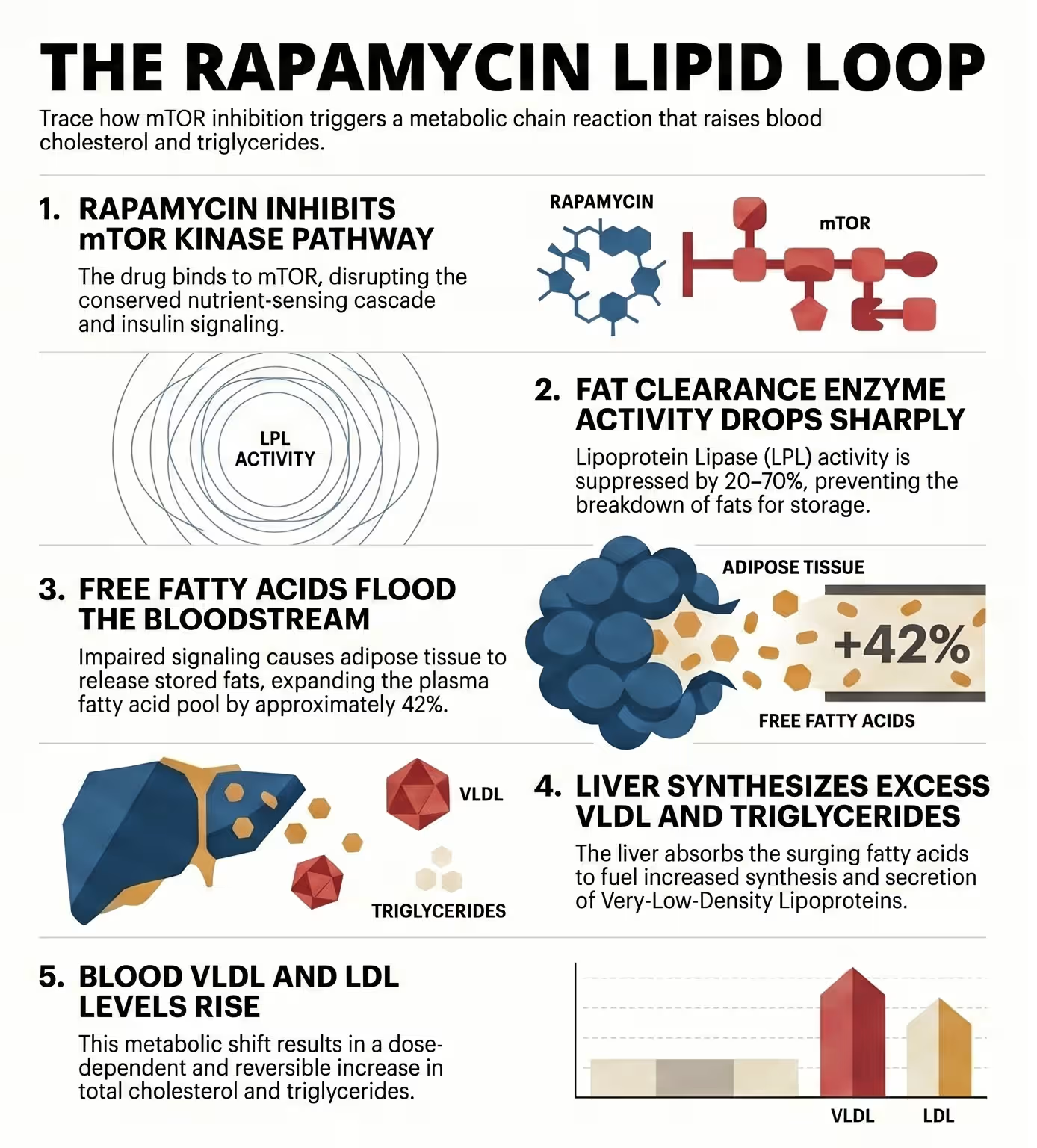
Rapamycin alters the insulin signaling pathway, which increases adipose tissue lipase activity and decreases lipoprotein lipase (LPL) activity. This results in the liver synthesizing more triglycerides and secreting more VLDL. Essentially, it expands the body’s free fatty acid pool, providing more substrate for lipid production [13].
The mechanistic driver of these lipid changes is the inhibition of the mTORC1 and mTORC2 complexes. Chronic treatment with rapamycin can disrupt the assembly of mTORC2 in tissues like the liver and muscle [2] [6]. This disruption leads to a state of “benevolent pseudo-diabetes,” where the body mimics a starvation state by shifting metabolism toward lipid mobilization and gluconeogenesis [10].
Morrisett et al. (2002) observed that sirolimus increased the mean plasma free fatty acid levels by over 40% [13]. While this can lead to elevated lipid markers on a blood test, it is often viewed by researchers like Blagosklonny as a protective “starvation-mimetic” response that may actually be required for the drug’s longevity effects [11] [14].
How Significant Are Lipid Changes at a Weekly Longevity Dose Compared to Daily Transplant Dosing?
Weekly longevity doses (e.g., 5-10 mg/week) typically cause much milder lipid elevations than daily transplant dosing (2-5 mg/day). In the PEARL trial, which followed healthy adults for one year on weekly doses, biomarkers remained within normal ranges, and no significant lipid-related adverse events led to study withdrawal [1].
The difference lies in “trough” versus “peak” exposure. Daily dosing maintains high levels of rapamycin that constantly suppress LPL activity, leading to sustained hyperlipidemia [9]. Weekly dosing allows for periods where mTOR function can partially recover, restoring normal lipid processing [10].
In the 48-week PEARL trial, participants receiving 5 mg or 10 mg weekly did not show significant changes in visceral adiposity, and their comprehensive blood panels remained stable. This suggests that the “pulse” protocol used for longevity avoids the severe hypertriglyceridemia seen in the transplant population [1].

Which Dietary Changes or Supplements Are Best for Managing Rapamycin-Induced Dyslipidemia?
Reducing simple carbohydrate intake and increasing high-quality fats (like Omega-3s) can help offset triglyceride spikes. Because rapamycin-induced lipid changes are driven by altered insulin signaling, diets that improve insulin sensitivity—such as ketogenic or low-carb protocols—are theoretically synergistic [10].
Managing lipids while on rapamycin requires a multi-faceted approach:
- Dietary Restriction: Combining intermittent rapamycin with intermittent fasting or very low-calorie diets (VLCD) may counteract potential hyperglycemia and lipid issues [10].
- Metformin: Often paired with rapamycin to improve insulin sensitivity and mitigate glucose intolerance [10].
- Lifestyle: Regular physical exercise is recommended to utilize mobilized free fatty acids as fuel for muscle tissue [11] [14].
Can Omega-3 Fatty Acids or Statins Be Taken Safely Alongside Rapamycin?
Yes, Omega-3 fatty acids and statins are commonly used alongside rapamycin to manage dyslipidemia. Statins do not generally interfere with rapamycin’s lifespan-extending properties in animal models, though they may have sex-dependent effects on health outcomes [11] [15].
Do Low-Carbohydrate or Ketogenic Diets Help Offset Rapamycin’s Effect on Triglycerides?
Theoretical evidence suggests they do, as ketogenic diets (KD) also induce a state of “benevolent pseudo-diabetes” that focuses on lipid utilization rather than glucose. Combining KD with rapamycin may stabilize blood glucose, though clinical trials in humans are still needed to confirm the long-term effects of this combination [10].
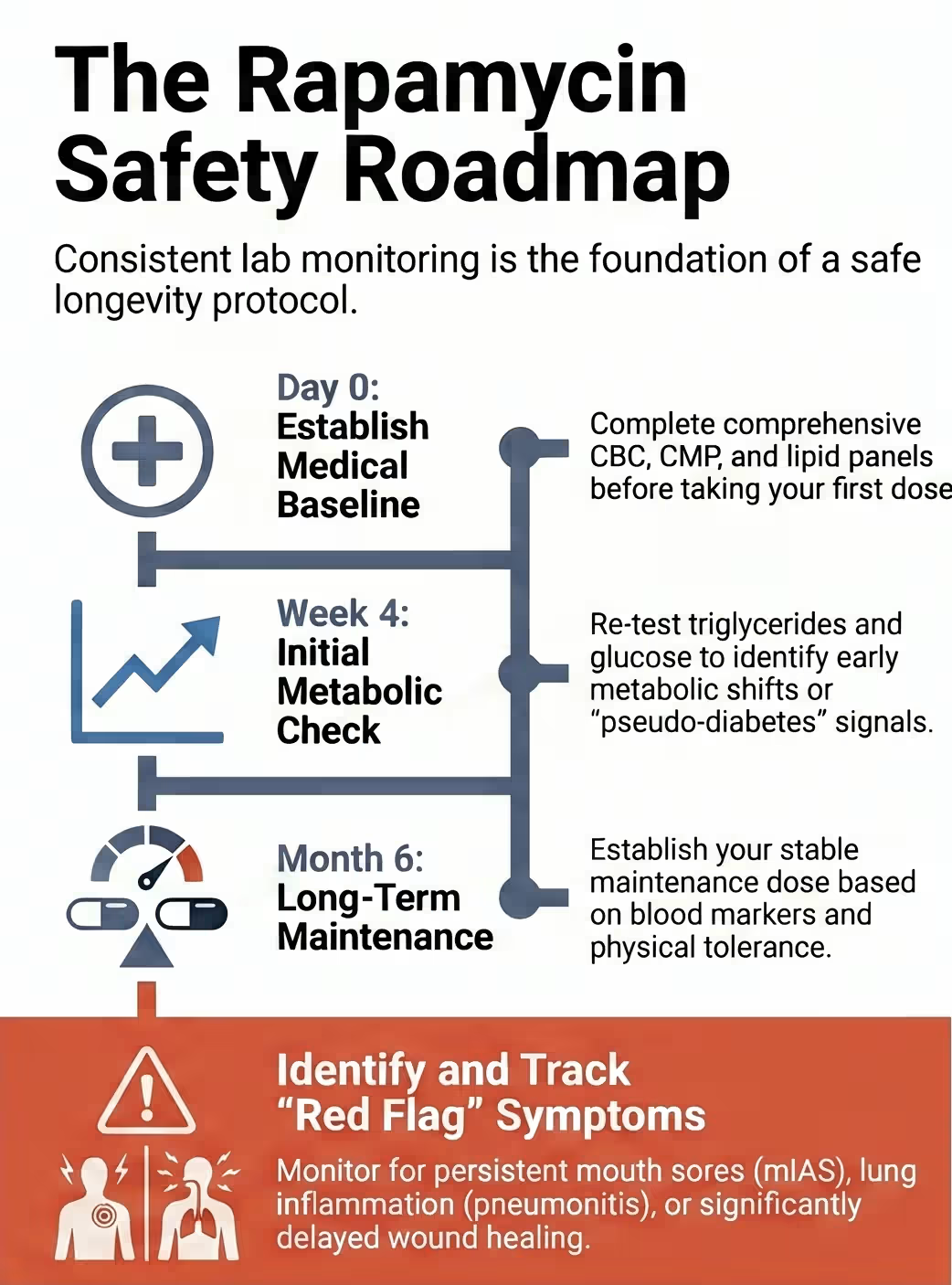
How Does Rapamycin Affect Blood Glucose and Insulin Resistance — Should You Test HbA1c?
Direct Answer: Chronic high-dose rapamycin can induce insulin resistance and elevate blood glucose, a condition often called “starvation pseudo-diabetes”. In healthy adults, low-dose rapamycin generally does not cause significant hyperglycemia [10] [11]. However, testing HbA1c is essential for monitoring long-term glucose stability and identifying potential metabolic shifts early [1].
Who Is Most at Risk for Significant Metabolic Side Effects from Rapamycin?
Patients with pre-existing obesity, metabolic syndrome, or a history of diabetes are at higher risk for metabolic disturbances. Paradoxically, some studies showed that patients without a prior history of diabetes developed mIAS more quickly, suggesting that metabolic background impacts side effect trajectory. Users taking calcineurin inhibitors or high-dose steroids also face increased risk [6] [10].
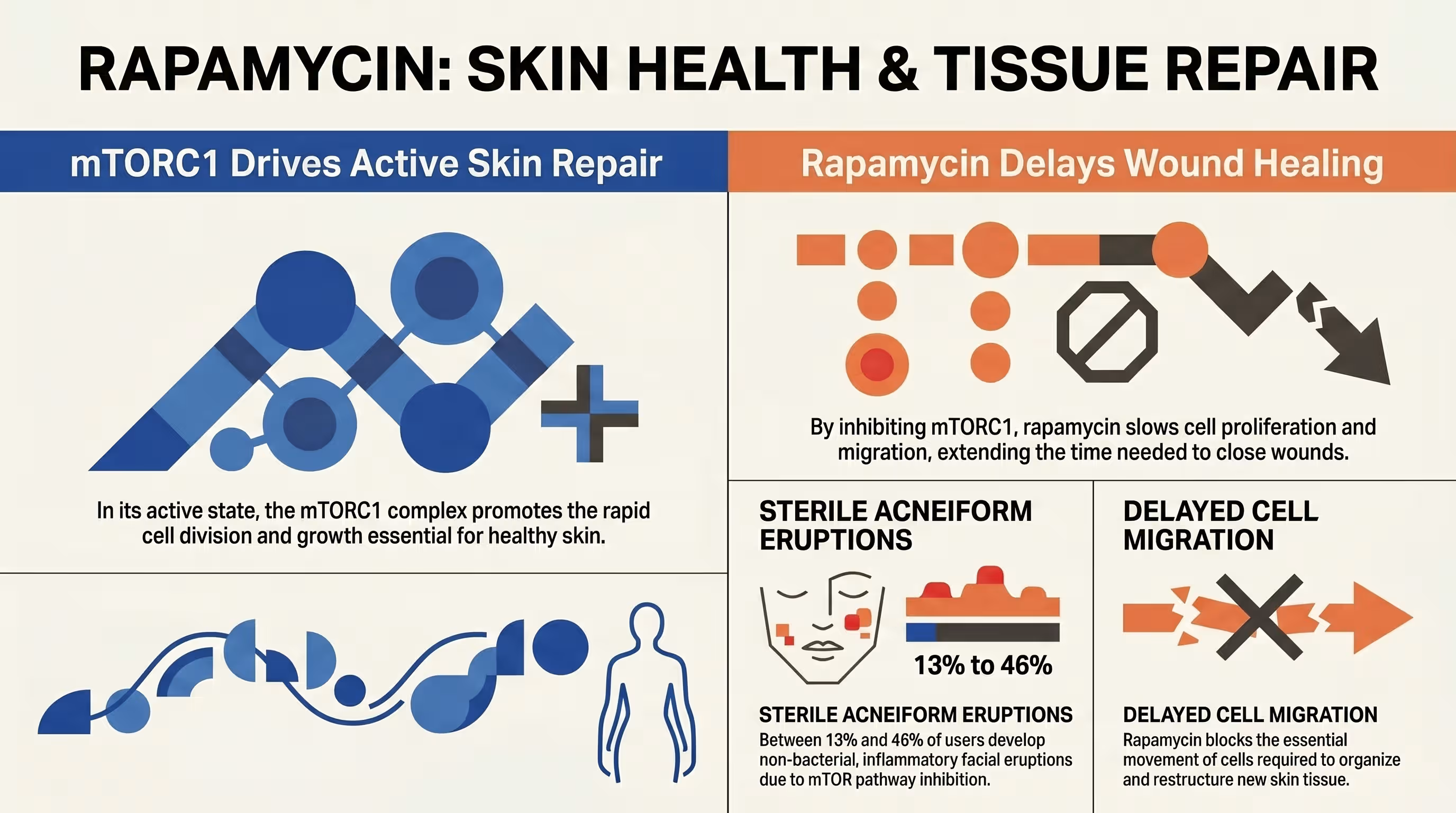
Does Rapamycin Cause Skin Rashes, Acne, or Wound-Healing Problems — and How Do You Manage Them?
Acneiform eruptions occur in 13-46% of rapamycin users and are typically sterile, inflammatory lesions on the face or trunk [16]. Because rapamycin is cytostatic and inhibits cell proliferation, it can also slow wound healing [13]. Managing these effects involves diligent skin care, monitoring for bacterial infections, and pausing the drug before major surgeries [11] [17].
What Does Rapamycin-Related Acneiform Rash Look Like, and Is It Different from Regular Acne?
Rapamycin-induced rashes present as folliculocentric red papules, often appearing in seborrheic areas like the face and back. Unlike regular acne, these eruptions typically lack comedones (blackheads/whiteheads) or cysts and are usually negative for bacterial cultures. They are often pruritic (itchy) and can recur upon drug re-initiation [4] [16].
Does Rapamycin Cause Hair Loss or Skin Changes in Women, and How Frequent Is This at Low Doses?
Hair loss (alopecia) and skin changes like fragile, ridged nails are recognized side effects, though they are much rarer at low longevity doses [17]. In the PEARL trial, women receiving 10 mg weekly actually reported significant improvements in pain and no major patterns of skin/hair distress were highlighted as study-stopping events [1].
Why Does Rapamycin Slow Wound Healing — and How Long Before Surgery Should You Stop Taking It?
Rapamycin inhibits mTOR, which is a master regulator of the cell growth and protein synthesis necessary for tissue repair [6] [12] [13]. For anti-aging purposes, it is generally advised to pause rapamycin for at least 2-3 weeks before and after major surgery to ensure optimal healing [11].
Can Rapamycin Cause Swelling or Edema in the Legs and Feet, and What Does This Signal?
Peripheral edema (swelling) is a known but less common side effect [17]. While it can signal fluid retention issues, it is often a benign, dose-dependent reaction. Persistent swelling should be reviewed by a physician to rule out more serious complications like venous issues or pneumonitis [11].
Is Rapamycin-Related Pneumonitis (Lung Inflammation) a Real Risk at Longevity Doses?
Non-infectious interstitial pneumonitis is a rare but serious side effect that requires immediate discontinuation of the drug. While primarily seen at high oncology doses, users should watch for “warning signs” like a new, unexplained cough or shortness of breath [11].
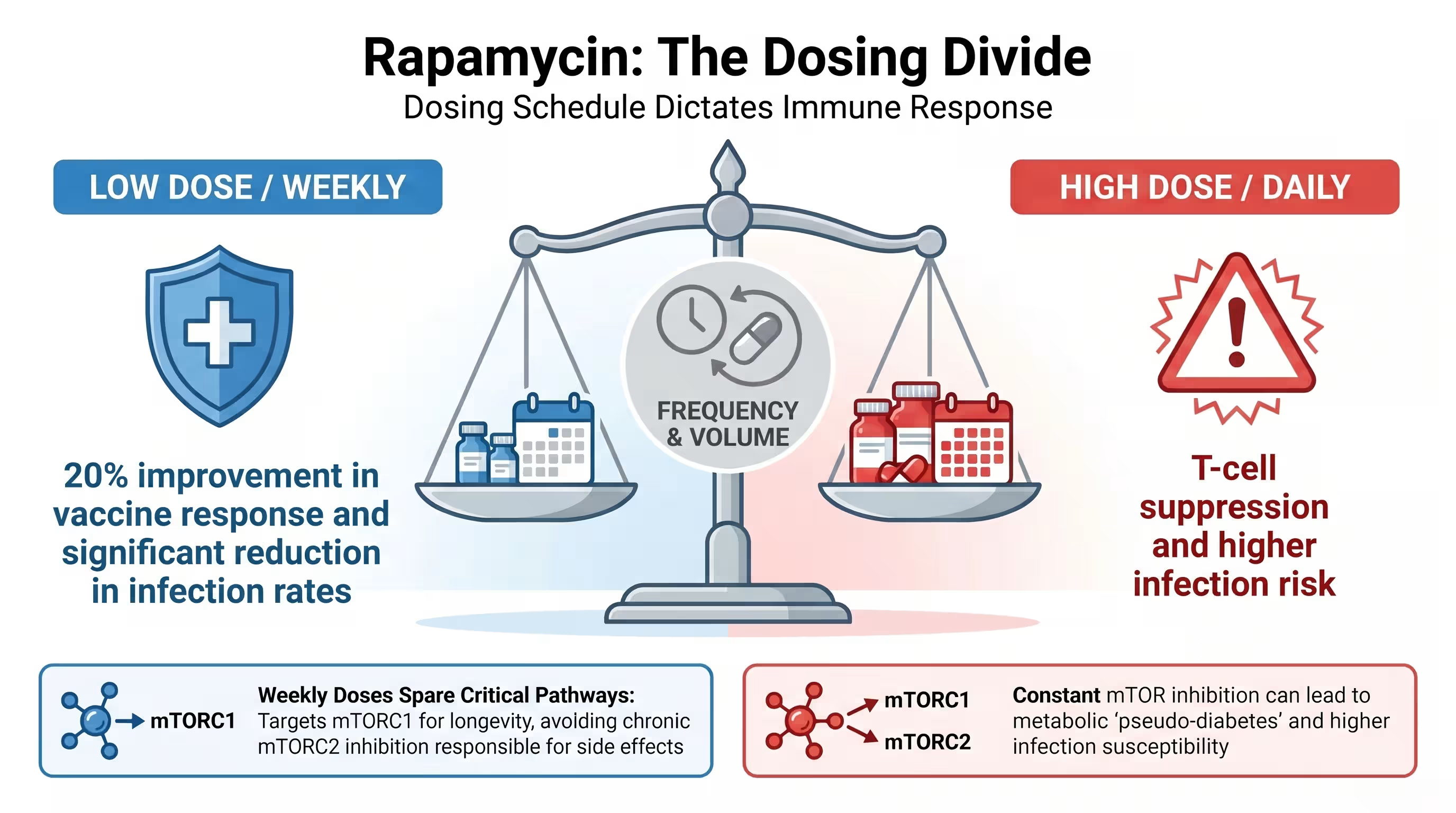
Will Rapamycin Suppress Your Immune System — and Is the Risk Real at Weekly Longevity Doses?
At low, intermittent doses, rapamycin acts as an immunomodulator that can actually enhance immune function in the elderly [10]. While high daily doses are used for immunosuppression in transplant patients, longevity protocols (like 5 mg/week) have been shown to improve the response to influenza vaccines and reduce the rate of infections [9] [18].
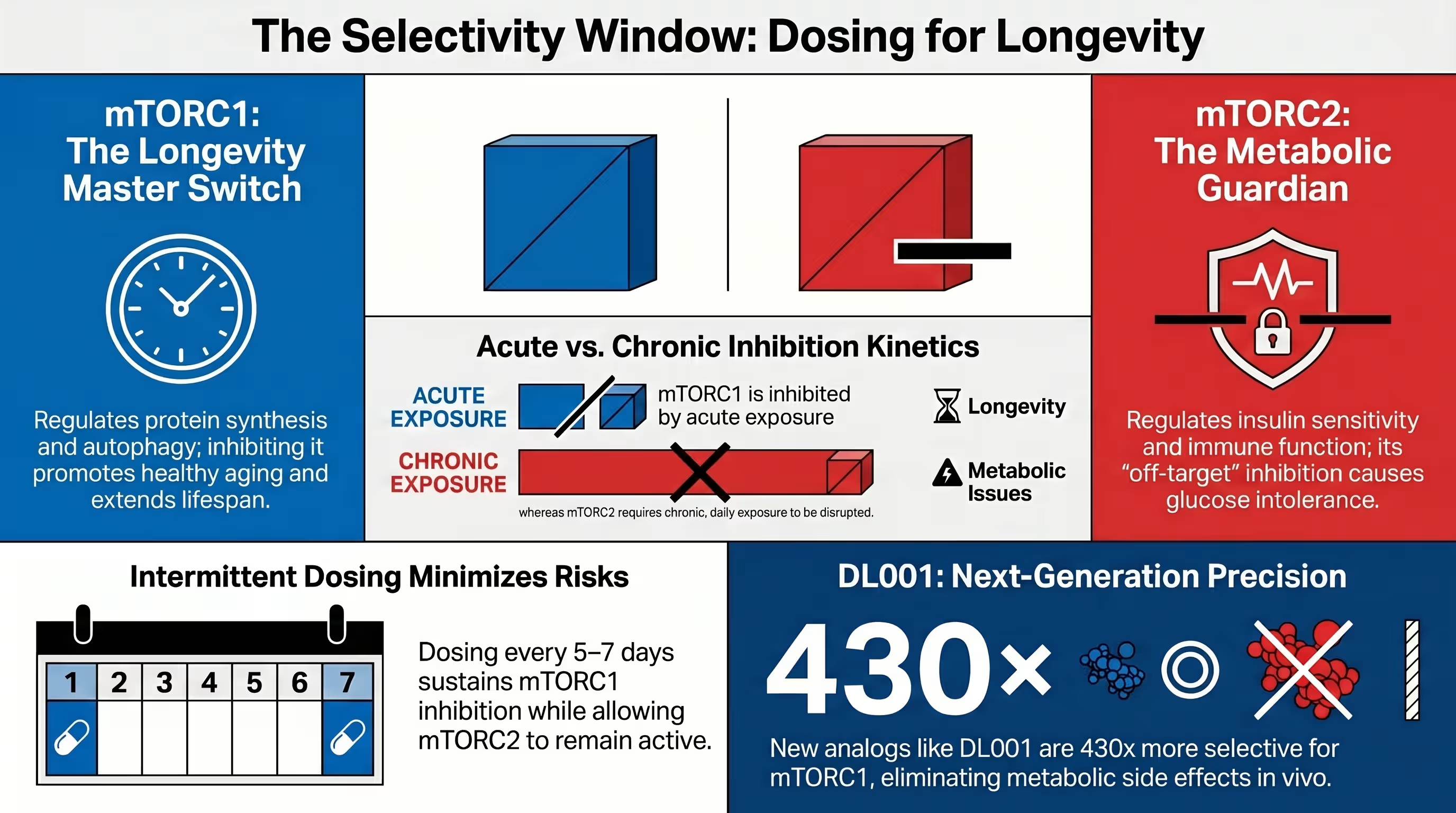
What Is the Difference Between mTORC1 and mTORC2 Suppression — and Why Does It Determine Your Infection Risk?
mTORC1 inhibition is largely responsible for the drug’s anti-aging benefits, while mTORC2 inhibition is associated with metabolic side effects and potential immune suppression. Low-dose regimens aim to selectively inhibit TORC1 while leaving TORC2 activity intact, which maintains T-cell function and reduces infection risk [2] [18].
mTORC1 regulates protein synthesis and autophagy; inhibiting it mimics calorie restriction [12]. mTORC2 is involved in cytoskeletal organization and insulin sensitivity. Prolonged exposure to high doses of rapamycin eventually disrupts the assembly of both complexes [2] [6].
Research by Mannick et al. (2018) demonstrated that low-dose catalytic mTOR inhibitors combined with rapalogs could achieve complete TORC1 inhibition without impacting TORC2. This “selective” approach was associated with a significant decrease in the rate of infections reported by elderly subjects over a one-year period [18].
Is It Safe to Get a Flu Shot, COVID Vaccine, or Other Vaccination While Taking Rapamycin?
Yes, and evidence suggests rapamycin may even make vaccines more effective in older adults [6] [15]. Mannick et al. (2014) found that 5 mg of a rapalog weekly enhanced the vaccine response by 20% by reducing the percentage of “exhausted” T cells that express the PD-1 receptor [9].
Does Rapamycin Affect Hormones or Menstrual Cycles in Women?
At immunosuppressive doses, side effects like menstrual irregularities and ovarian dysfunction have been reported [12]. However, for healthy, post-menopausal women, the PEARL trial showed rapamycin was well-tolerated and even improved self-reported pain and lean muscle mass [1].
Who Should Absolutely Not Take Rapamycin Because of Immune or Infection Risk?
Individuals with active serious infections, a history of chronic open wounds, primary immune deficiency, or those undergoing chemotherapy should avoid rapamycin [1]. Because it can inhibit neutrophil function, it may increase the severity of bacterial infections if used improperly [11].
When Should You Stop Rapamycin — What Are the Warning Signs That Require Immediate Medical Attention?
Stop rapamycin immediately and seek medical attention for:
- Shortness of Breath or New Cough: Possible signs of pneumonitis [11].
- Severe Sore Throat or High Fever: May signal a serious infection [1].
- Visible Open Sores That Don’t Heal: Signals impaired wound repair [1].
- Signs of Allergic Reaction: Such as angioedema or hives [17].
Conclusion
The most common rapamycin side effects—mouth sores and lipid changes—are well-understood, reversible, and manageable for the majority of users. By utilizing a pulsatile weekly dosing protocol, maintaining diligent lab monitoring, and using topical steroids when necessary, users can likely access the drug’s profound longevity benefits while minimizing risk.
Key Takeaways:
- mIAS is not regular mucositis: It resembles canker sores and is best treated with topical dexamethasone rinses.
- Lipids will likely rise: This “starvation-mimetic” effect is dose-dependent and reverses quickly upon stopping the drug.
- Immune effects are biphasic: High daily doses suppress immunity, but low weekly doses can enhance it in older adults.
- Monitoring is non-negotiable: Baseline and periodic blood tests for lipids, CBC, and glucose are essential for safety.

No, survey data of off-label users actually found that rapamycin was associated with lower rates of depression and anxiety compared to non-users.
It is generally advised to pause rapamycin during active bacterial or viral infections to ensure the immune system is fully capable of responding to the pathogen.
Alopecia is a rare side effect primarily seen at high, daily doses; it was not a significant finding in the PEARL trial using weekly longevity doses.
Yes, clinical trials in healthy older women showed significant improvements in lean muscle mass and pain levels with few reported serious adverse events.
Yes, CBD is a potent inhibitor of the enzyme that breaks down rapamycin, which can lead to dangerously elevated blood levels and increased toxicity.
RapaShop.net offers a trusted, high-quality source for rapamycin. RapaShop is familiar with the needs of the rapamycin community and provides a streamlined purchasing experience.
Resource links
[1] Influence of rapamycin on safety and healthspan metrics after one year: PEARL trial results
[2] mTORC2 takes the longevity stAGE
[3] Management of mTOR inhibitors oral mucositis: current state of knowledge
[8] Evaluation of off-label rapamycin use on oral health
[9] mTOR inhibition improves immune function in the elderly
[10] Fasting and rapamycin: diabetes versus benevolent glucose intolerance
[11] Rapamycin for longevity: opinion article
[12] Rapamycin for longevity: the pros
[13] Effects of sirolimus on plasma lipids
[14] About-face on the metabolic side effects of rapamycin
[15] Evaluation of off-label rapamycin use to promote healthspan in 333 adults
[16] Acneiform Eruptions Possibly Triggered by Clarithromycin During Sirolimus Treatment
[18] TORC1 inhibition enhances immune function and reduces infections in the elderly