Combining Rapamycin with Other Longevity Interventions: Metformin, NAD+, and More

Researchers now pursue human longevity through synergistic protocols instead of single-drug solutions. These combinations target the complex network of aging hallmarks simultaneously.
Rapamycin remains the most effective drug for extending mammalian lifespans. However, real-world users often “stack” it with other interventions. People combine it with metformin, NAD+ precursors, and lifestyle changes. These additions enhance both efficacy and safety. [1]. This guide explores the advanced mechanisms, recent 2026 clinical findings, and nuanced user protocols for combining these powerful geroprotectors [2] [3].
Rapamycin Combination Overview
Why people stack rapamycin with longevity interventions?
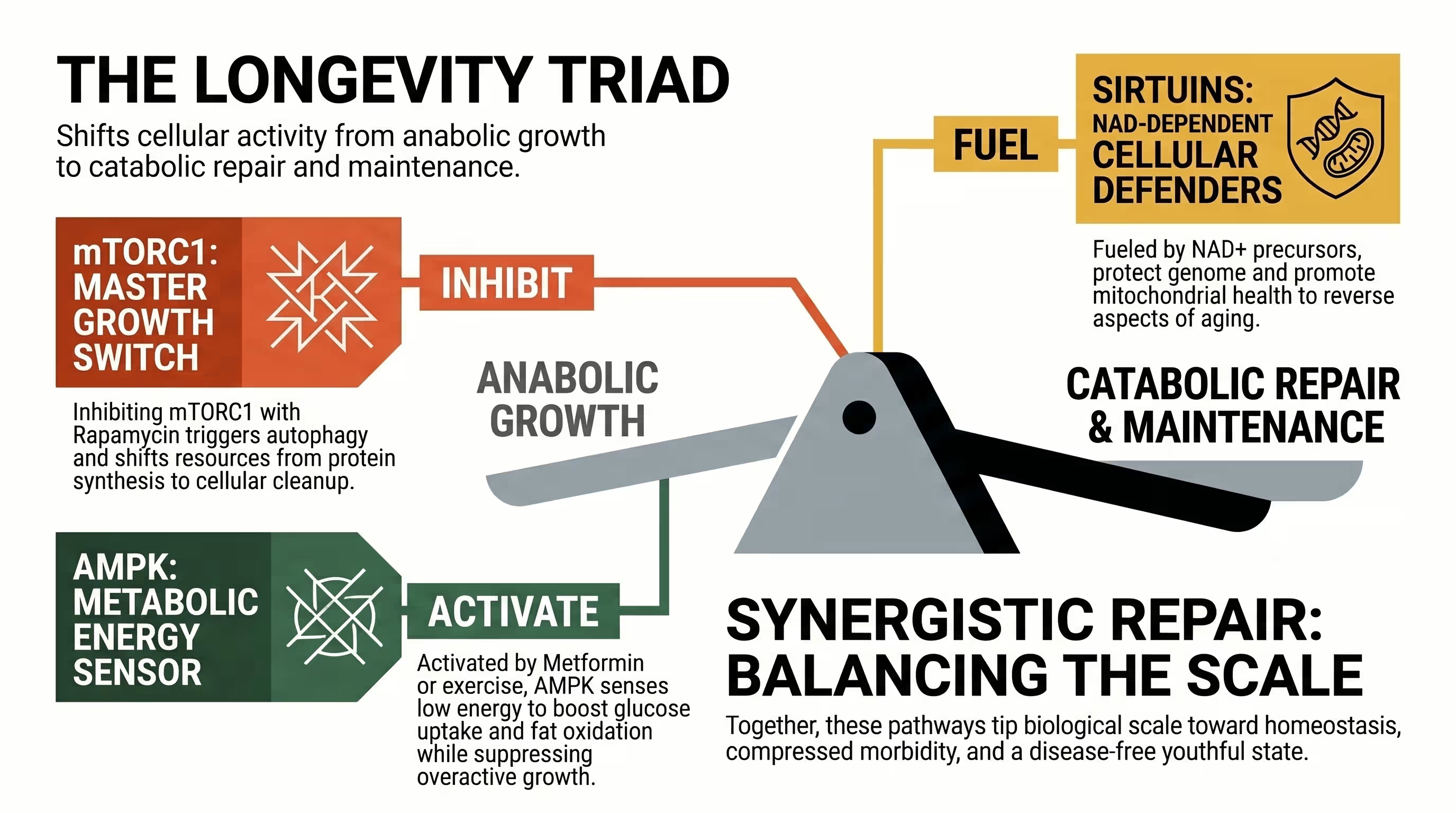
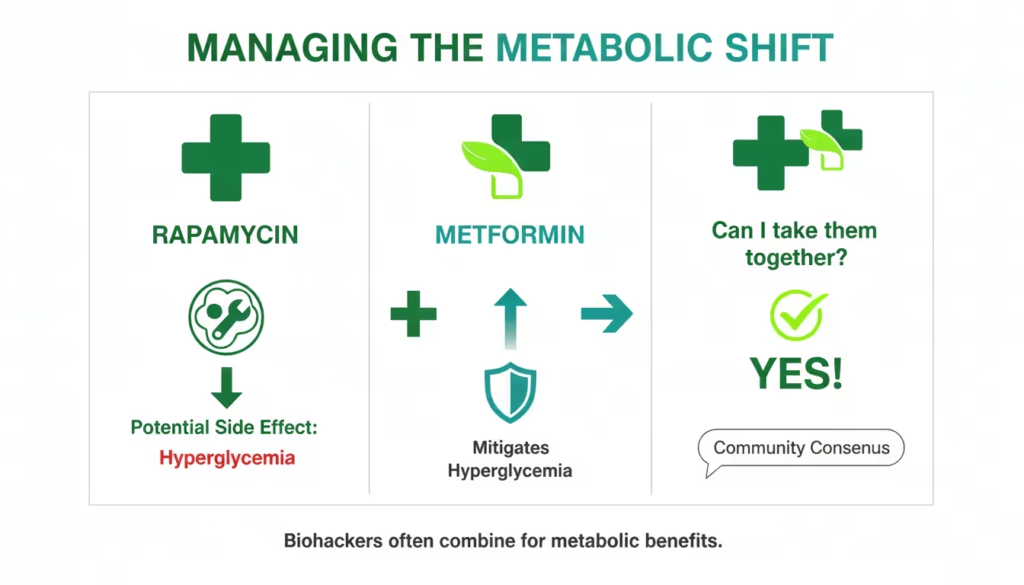
Stacking rapamycin with other interventions aims to achieve synergistic healthspan extension by simultaneously modulating multiple nutrient-sensing pathways like mTOR, AMPK, and sirtuins [4]. This multi-targeted approach potentially offers greater benefits than any single agent. It uses compounds like metformin to counteract metabolic disruptions from rapamycin. For instance, metformin prevents glucose intolerance [5] [6].
The biological process of aging is not driven by a single “broken” pathway but by an interconnected network of cellular damage and signaling shifts [6]. Rapamycin is highly effective because it inhibits mTORC1, a master regulator that, when overactive, accelerates aging by promoting cellular growth at the expense of repair [7]. However, aging also involves the decline of energy sensors like AMPK and the depletion of vital metabolites like NAD+ [4] [7].
By combining rapamycin with an AMPK activator (metformin) and an NAD+ booster, users attempt to reallocate cellular energy from wasteful proliferation to somatic maintenance and autophagy [4] [8]. Strategic stacking also addresses the “off-target” effects of rapamycin [8] [5]. While inhibiting mTORC1 is beneficial, chronic rapamycin use can unintentionally inhibit mTORC2, leading to insulin resistance and lipid imbalances [7] [2] [9]. Stacking allows for protocols that maintain high sensitivity to insulin while still capturing the lifespan-extending benefits of mTOR inhibition [6] [9].

How rapamycin differs from metformin, NAD+, fasting, and exercise?
Rapamycin is a direct inhibitor of mTORC1, acting as a potent “brake” on cellular growth and a powerful inducer of autophagy [10] [11]. Metformin and fasting primarily activate the AMPK pathway. This process triggers cellular energy regulation and metabolic health.In contrast, exercise provides a physiological stimulus for renewal. It promotes both anabolic growth and catabolic breakdown. Finally, NAD+ precursors support essential cellular maintenance. They fuel sirtuin-mediated DNA repair and enhance mitochondrial function. [12] [13] [14].
Understanding these differences is critical for designing an effective stack. Rapamycin’s mechanism is unique because it forms a complex with the protein FKBP12 to physically block mTORC1 activity [6] [2] [15]. This is a direct “top-down” approach to slowing the aging clock [7] [10]. Metformin uses a “bottom-up” approach. It moderately inhibits mitochondrial complex I and increases the AMP/ATP ratio. The change triggers AMPK. Finally, AMPK indirectly turns down mTOR signaling [7] [16].
Lifestyle interventions like fasting and exercise provide the most natural modulation of these pathways [14]. Fasting mimics a nutrient-scarce environment. Rapamycin targets this same biological pathway through pharmacological means.
Exercise stands alone as the only intervention that squares the longevity curve. It improves cardiorespiratory fitness and increases muscle strength. These two factors serve as the strongest predictors for long-term survival [6] [1]. NAD+ precursors, such as NMN or NR, provide the “fuel” for sirtuins to perform essential deacetylation tasks that protect the genome and maintain metabolic flexibility [4] [17].
Rapamycin and Metformin
Mechanistic overlap: AMPK, mTOR, and metabolic health
Rapamycin and metformin overlap at the mTOR/AMPK signaling hub, where they work in tandem to suppress overactive growth signals and restore metabolic homeostasis [4] [10]. Rapamycin directly shuts down the anabolic mTORC1 pathway. Meanwhile, metformin activates the catabolic AMPK pathway. This activation further inhibits mTORC1. It also promotes mitochondrial biogenesis and glucose uptake [12] [16].
Researchers often call this combination the “ITP Stack.” The National Institute on Aging’s Interventions Testing Program (ITP) tested these two drugs together. The study demonstrated a significant increase in median lifespan for mice. This combination potentially exceeds the life-extending effects of rapamycin alone [8] [18] [6]. The primary reason for this synergy is that they attack cellular aging from two different angles within the same metabolic circuit [4] [7].
Metformin functions as a gerosuppressant by increasing the activity of sestrins, which are proteins that integrate stress inputs to inhibit mTOR [16]. Additionally, metformin has been shown to reduce the “transcriptional noise” that accumulates with age, while rapamycin focuses on clearing the “cellular trash” through enhanced autophagy [11] [6] [7]. In 2026, researchers are increasingly focused on how this combination maintains proteostasis (protein balance) in tissues like skeletal muscle, which is vital for preventing age-related frailty [8] [1].
Can I take rapamycin and metformin together?
Yes, clinical and preclinical evidence suggests that rapamycin and metformin can be taken together, and this combination may be superior for longevity than either drug used in isolation [6] [8]. Data from 2025 and 2026 studies indicate that metformin is particularly effective at neutralizing the glucose intolerance and weight loss sometimes caused by frequent rapamycin dosing [1] [6].
You can take these two drugs together. However, benefits depend on biological sex and the specific dosing regimen. In female mice, metformin almost completely cancels out the glucose intolerance from long-term rapamycin treatment [19]. In males, while metformin did not reverse glucose intolerance in some studies, it did prevent rapamycin-mediated reductions in insulin and leptin, suggesting a stabilization of metabolic hormones [6].
For human users, the decision to combine them often hinges on metabolic monitoring [2] [20]. If a user’s blood glucose or HbA1C levels rise after starting a rapamycin protocol, metformin is frequently added to restore insulin sensitivity [20] [6]. Some experts still doubt metformin’s benefits for metabolically healthy people. These individuals already maintain their health through diet and exercise. In this specific context, the drug might not provide extra anti-aging value [7].
Potential benefits, tradeoffs, and use cases
The rapamycin & metformin stack extends lifespan and preserves metabolic health. However, users may experience gastrointestinal side effects. The stack might also blunt exercise-induced mitochondrial adaptations [6] [5] [14]. Use cases typically involve individuals with signs of insulin resistance or those using higher, more frequent rapamycin doses that necessitate metabolic support.
| Feature | Rapamycin (Sirolimus) | Metformin | Combined Stack |
|---|---|---|---|
| Primary Target | mTORC1 | AMPK | Dual mTOR/AMPK |
| Lifespan Impact | High (ITP Proven) | Inconclusive/Small | Potentially Highest |
| Glucose Impact | May cause intolerance | Improves sensitivity | Normalized glucose |
| Best Use Case | Longevity / Anti-cancer | Diabetes / Metabolic health | Optimized Longevity |
| Common Side Effect | Mucosal ulcers / Lipids | GI distress / B12 deficiency | Synergistic GI risk |
Monitoring: glucose, insulin resistance, and lipids
Users of a rapamycin and metformin stack should conduct quarterly blood panels to monitor fasting glucose, HbA1C, and lipid profiles (Total/LDL cholesterol and triglycerides) [21]. Monitoring for a rise in triglycerides is essential because rapamycin can inhibit mTORC2. You must also track any decrease in albumin. These markers help you assess whether the dosing frequency is too high [20] [7].
Monitoring should go beyond basic labs to include HOMA-IR (Homeostatic Model Assessment for Insulin Resistance), which provides a more accurate picture of how well the body is handling glucose [2] [6]. Recent 2025 research suggests checking blood rapamycin levels regularly to ensure levels stay within a “geroprotective” range. This range typically spans 5 to 15 ng/mL. Monitoring prevents the drug from reaching toxic or immunosuppressive concentrations [3] [20].
If lipids like LDL cholesterol rise—a common side effect of rapamycin—some practitioners may adjust the dose or timing rather than adding a third drug like a statin [7] [2]. Metformin primarily acts as a metabolic stabilizer in this context. It prevents rapamycin-induced glucose intolerance from progressing into clinical type 2 diabetes. This ensures that the mild metabolic shifts remain manageable and safe for the patient [11] [10] [18].
Rapamycin and NAD+
What NAD+ precursors are trying to support?
NMN and NR serve as NAD+ precursors. Precursors aim to restore cellular levels of NAD+ in the body. This vital coenzyme naturally declines as you age. It is essential for the proper function of sirtuins [4] [17]. Higher NAD+ levels support mitochondrial energy production, DNA repair, and systemic metabolic flexibility [6] [4].
NAD+ is the essential “fuel” for SIRT1, a sirtuin that regulates aging by deacetylating key proteins involved in stress resistance and metabolism [13]. Aging increases enzymes like CD38, which consume more NAD+. This leaves less NAD+ available for vital repair processes. Precursor supplements help “refill the tank” by boosting these levels. This allows sirtuins to maintain youthful gene expression patterns [4].
The “Senolytics NAD+ Rapamycin Stack” aims for a complete cellular reset. Rapamycin triggers autophagy to prevent the accumulation of damaged cellular components. Meanwhile, NAD+ precursors provide mitochondria with the energy to finish these recycling processes efficiently [11]. This is a dual-pathway strategy: rapamycin stops the “aging accelerator” (mTOR), and NAD+ precursors boost the “repair crew” (Sirtuins) [4].
Where NAD+ and rapamycin may complement each other?
NAD+ and rapamycin complement each other by balancing the “Tango” between sirtuins and mTOR [17]. SIRT1 negatively regulates mTOR. Boosting NAD+ helps keep mTOR in check naturally. Rapamycin provides direct pharmacological inhibition. This inhibition captures maximal longevity benefits [13] [4].
Mechanistically, SIRT1 interacts with TSC2, an upstream inhibitor of mTORC1 [13]. High NAD+ levels increase SIRT1 activity. This process strengthens the TSC complex, which keeps mTORC1 suppressed. Consequently, NAD+ precursors may boost the effects of rapamycin. This synergy could allow lower drug doses to achieve the same life-extending results [6] [13] [4].
NAD+ and rapamycin offer complementary neuroprotective effects. Researchers have tested pretreatment with rapamycin, metformin, or NMN. These compounds reduce cognitive impairment following cerebral hypoperfusion. They work by inhibiting microglial phagocytosis. This process prevents the immune system from “eating” healthy brain cells [22] [6]. Stacking them may provide a multi-layered defense against neurodegenerative diseases like Alzheimer’s [11] [7].
Evidence limits and biomarker expectations
While animal data is robust, human evidence for the NAD+ and rapamycin stack is still emerging, and many benefits remain theoretical [11] [20]. Users should expect subtle shifts in biomarkers like DNA methylation (epigenetic) clocks or improved insulin sensitivity in muscle rather than immediate, dramatic physical changes [6] [23].
One significant hurdle is that intravenous NAD+ may have different effects than oral precursors, and the optimal human dose for longevity is unknown [6]. Some researchers, like Dr. Matt Kaeberlein, remain skeptical of the “hype” surrounding NAD+ boosters until more independent labs replicate the dramatic lifespan results seen in early studies [7].
For those stacking these interventions in 2026, biomarker expectations should be grounded in functional outcomes [2] [3]. Grip strength and walking speed provide reliable data on your longevity routine. Systemic inflammation markers like hs-CRP also offer consistent insights. These metrics outperform “biological age” tests. Such tests often fluctuate based on your immediate health status. Use these physical indicators to track your progress accurately [6] [23].

Rapamycin and Lifestyle Interventions
Rapamycin and fasting or intermittent fasting
Rapamycin and fasting are mechanistically similar, as both induce autophagy by suppressing nutrient-sensing signals through mTORC1 [20]. Many users coordinate rapamycin dosing with short-term fasting. Both methods target the same biological pathway. This strategy aims to maximize the autophagic peak. However, users must monitor the cumulative effect on muscle mass [23] [1].
Rapamycin is often called a “Dietary Restriction Mimetic” because it tricks the cell into thinking it is starving, even when nutrients are present [11] [18]. However, they are not identical [24]. Dietary restriction (DR) has a broader effect, downregulating genes involved in energy expenditure and shifting metabolism toward ketone body production (β-oxidation) [18]. Rapamycin focuses more narrowly on mTORC1 and protein translation [7] [10].
The 2026 research updates suggest that combining the two (Rapa + DR) results in a larger change in the liver transcriptome and metabolome than either alone, indicating synergistic benefits [24] [18]. For practical application, users often avoid dosing rapamycin during a “refeeding” phase to prevent interference with the anabolic signals needed for muscle recovery [23] [1].
Rapamycin and exercise
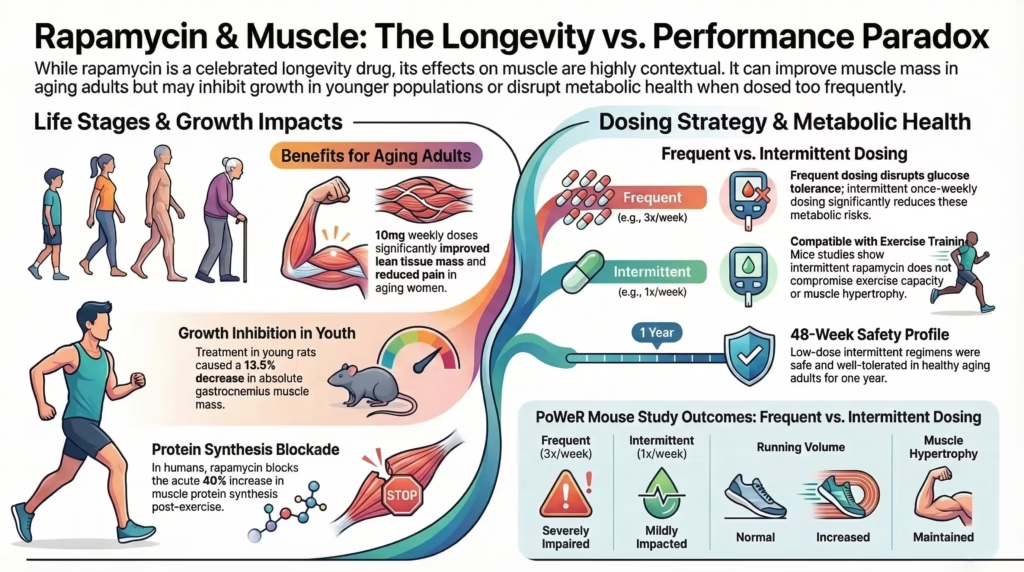
Contrary to previous “dogma” that rapamycin would blunt the benefits of physical activity, recent 2025 and 2026 studies show that rapamycin is largely compatible with voluntary exercise. While high, frequent doses can attenuate acute muscle protein synthesis, intermittent weekly dosing does not compromise physical performance, maximal exercise capacity, or absolute grip strength [1] [25].
The relationship between rapamycin and exercise revolves around the mTOR anabolic/catabolic cycle [23]. Exercise acutely activates mTOR to build muscle, while rapamycin inhibits it to induce repair [23]. New research studied adult female mice on intermittent rapamycin once per week. These mice ran a greater cumulative distance than others. They also showed significant muscle growth. This hypertrophy matched the results of the vehicle-treated control group [1] [25].
The key takeaway for 2026 is that timing and dosing frequency are the most important variables [2] [11]. Frequent dosing (3x/week) can disrupt the decline in adiposity (fat loss) normally seen with exercise, but weekly dosing preserves these metabolic benefits [1] [25]. This makes a strong case for “cycling” rapamycin rather than daily use for physically active adults [7] [11].
Rapamycin and muscle growth or hypertrophy
While rapamycin can acutely blunt the protein synthetic response to a single bout of resistance training, it does not necessarily prevent long-term muscle hypertrophy when used intermittently [1] [25] [20]. In fact, by reducing “inflamm-aging” and preventing sarcopenia in sedentary states, rapamycin may help preserve muscle quality as one ages [10] [23].
Muscle preservation is a major focus of human clinical trials. In rodent models of “PoWeR” (Progressive Weighted Wheel Running), rapamycin did not impede adaptations in muscle mass or myofiber size. This suggests that the body has compensatory signaling pathways (like mTORC2 or the MAPK pathway) that can drive muscle growth even when mTORC1 is periodically suppressed [1] [25].
Rapamycin and dietary restriction
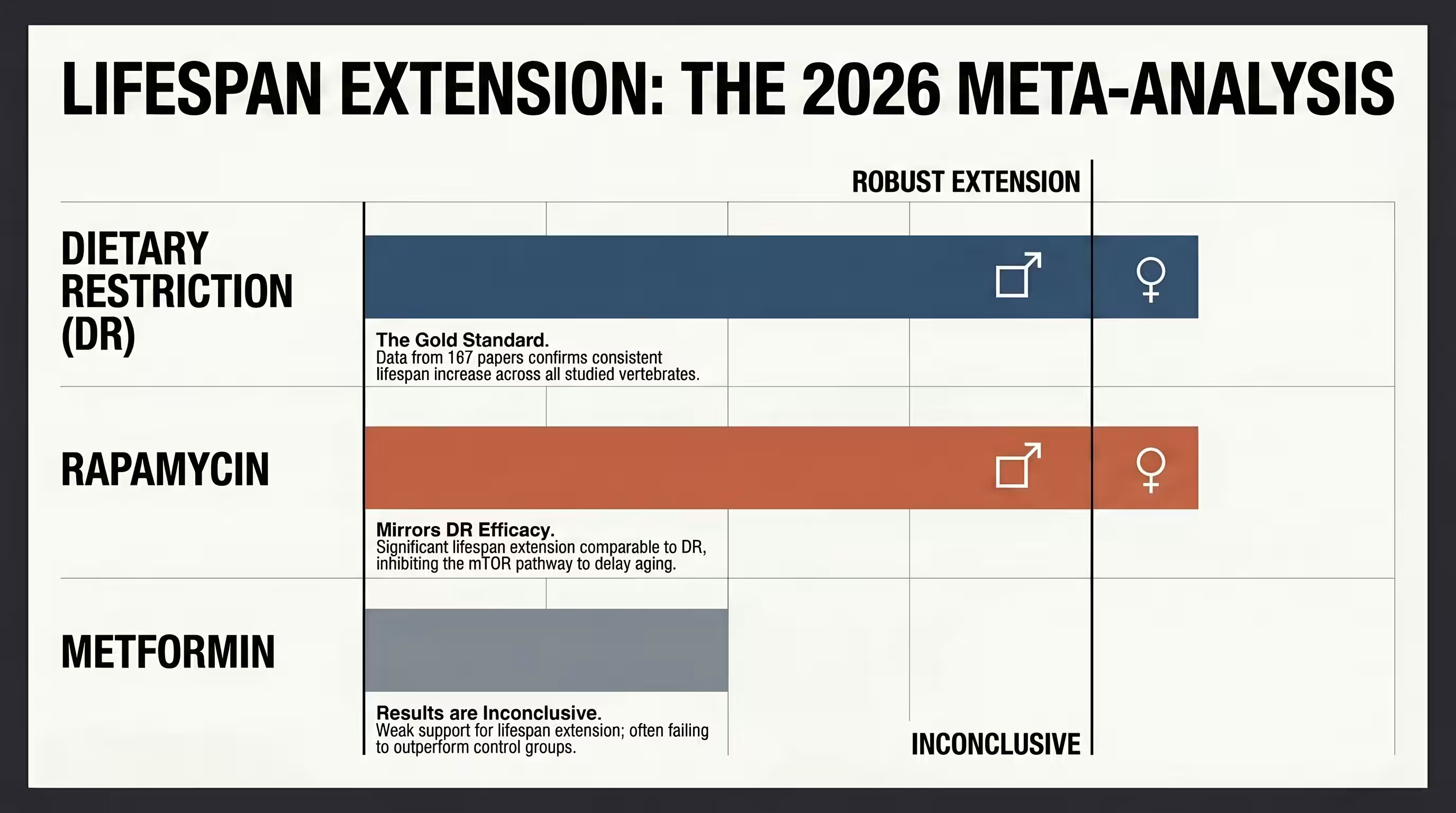
Rapamycin and dietary restriction (DR) are the two most robust longevity interventions, but they are not redundant [18] [19]. Meta-analyses in vertebrates show that rapamycin extends lifespans as effectively as dietary restriction. These two interventions affect over 80% of their target genes differently. This suggests that combining them will produce a greater effect than using either intervention alone [18] [19] [24].
While they both reduce mTOR signaling, DR also significantly reduces IGF-1 and leptin levels, which rapamycin typically does not. In 2026, the consensus is that rapamycin is not a “true” mimetic but a complementary agent. When combined, they have a synergistic effect on the liver transcriptome, increasing the number of significantly changed genes from roughly 2,500 to over 4,300 [18] [19] [24].
This synergy is also visible in epigenetic aging [23]. Both DR and rapamycin reduce the “epigenetic clock” (DNA methylation age), but DR typically shows a ~30% greater reduction. Combining them appears to “potentiate” these effects, creating a more youthful molecular signature [18] [24].
Dosing and Timing
Low-dose rapamycin and intermittent dosing
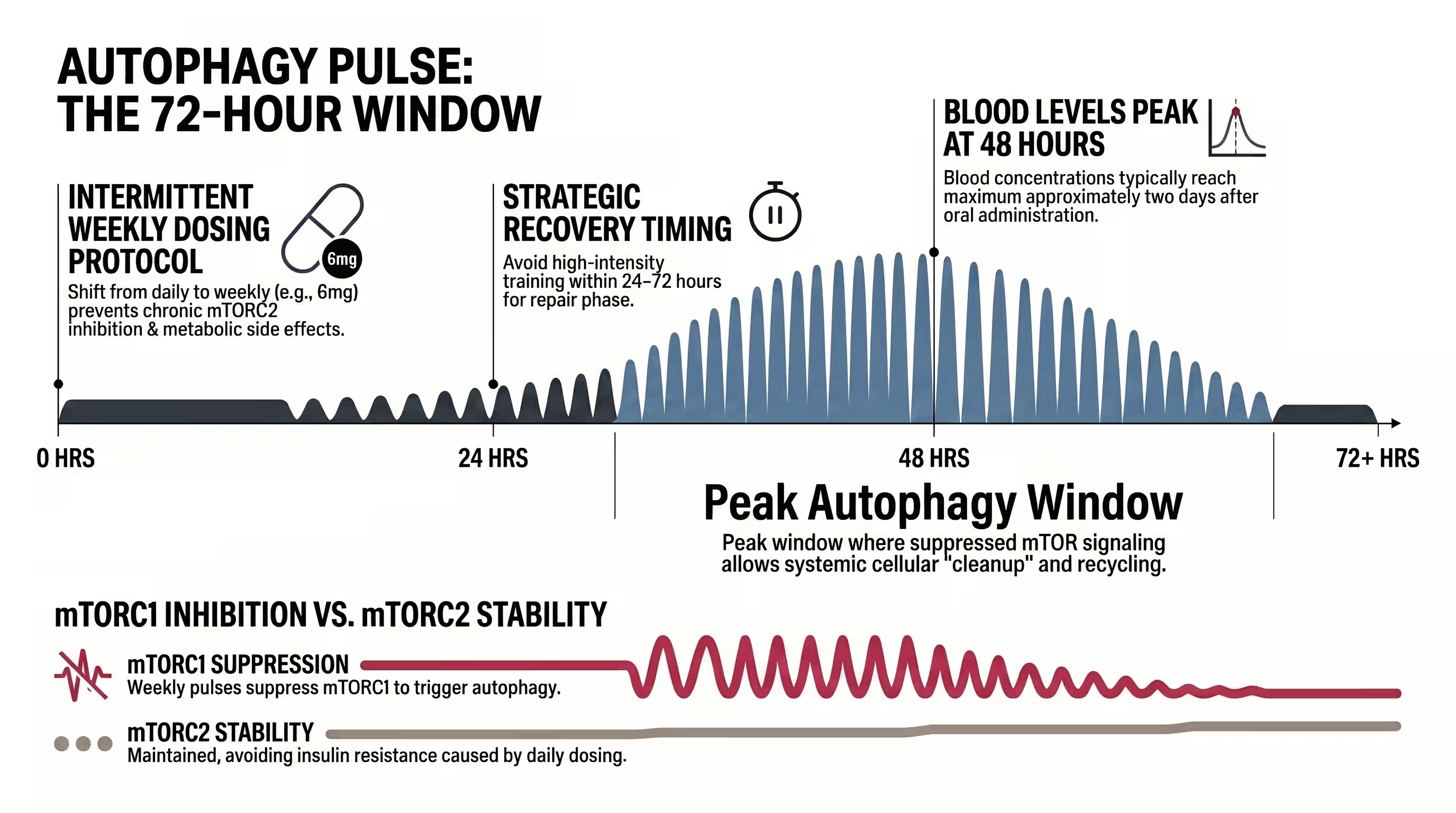
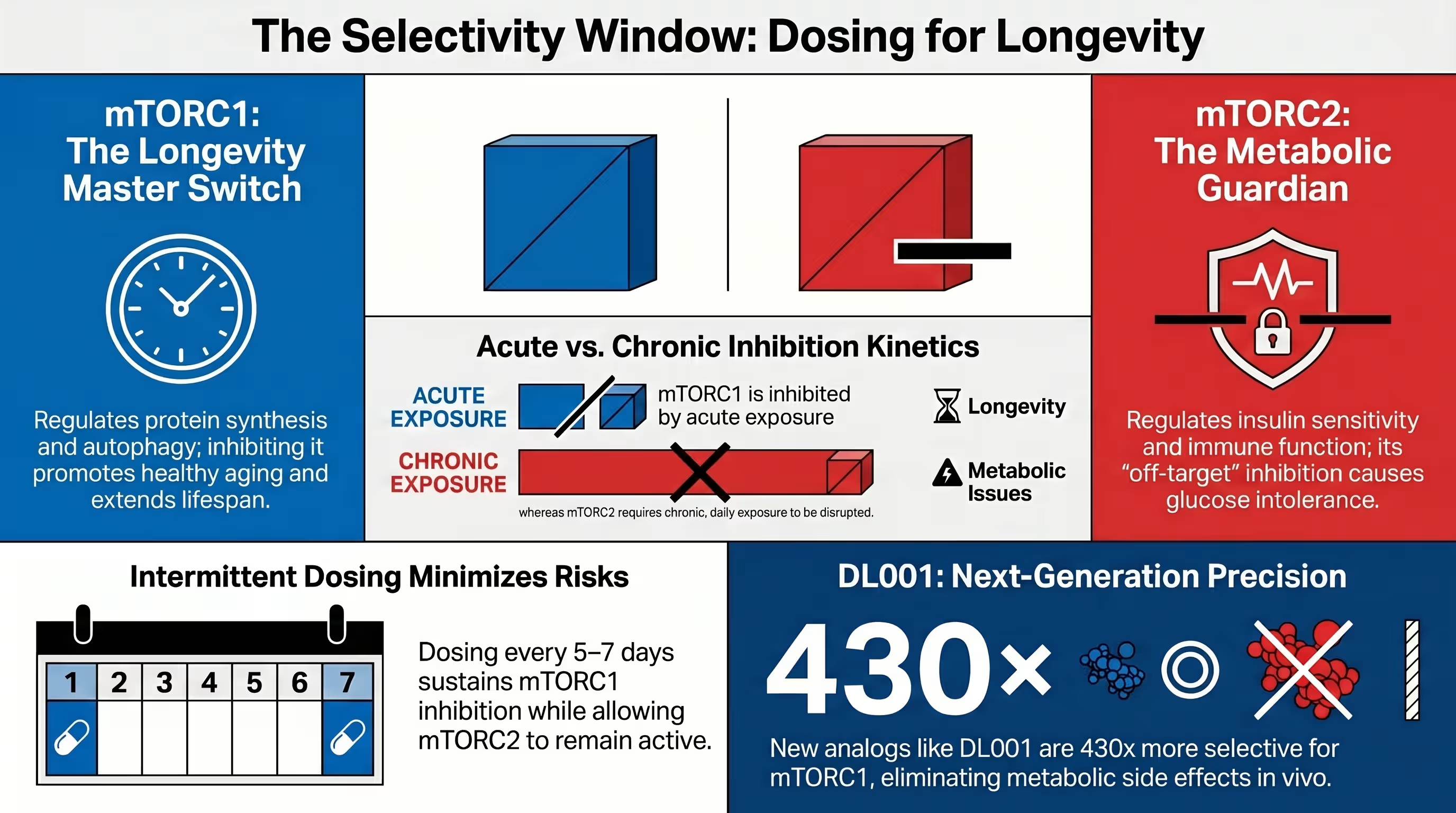
The modern longevity protocol has shifted away from daily use to low-dose intermittent dosing (e.g., 5-7 mg once weekly) [3] [20]. Intermittent dosing aims to maximize mTORC1 inhibition. It provides a “drug holiday” to let mTORC2 reconstitute. This approach avoids chronic immunosuppression and insulin resistance [2] [5] [11].
Intermittent dosing (e.g., 2 mg/kg weekly in mice) has been shown to extend lifespan while circumventing metabolic side effects [5] [7]. In humans, s cohort study in 2025 found that 6 mg per week was the most common dose reported by normative aging adults, with many self-reporting benefits in mood, pain, and cognition [3].
This weekly pulse allows for transient inhibition of mTORC1 in skeletal muscle, which typically returns to baseline within 72 hours, perfectly aligning with the recovery period between intense training sessions [1] [25].
Weekly sirolimus protocols in human studies
Current human trials use weekly doses ranging from 5 mg to 15 mg to identify the “Recommended Phase 2 Dose” (RP2D) [2]. For example, the PEARL trial randomized subjects to 5 mg or 10 mg weekly, while the RAP PAC trial tests up to 15 mg per week to evaluate safety and pharmacokinetics in healthy older adults [2] [11].
Human protocols are highly nuanced. The goal is to reach a trough level (the lowest drug level in the blood before the next dose) that is high enough to inhibit aging markers but low enough to avoid toxicity. Routine measurement of blood rapamycin levels is recommended, as there is significant inter-individual variability in how the drug is absorbed and metabolized [3].
| PEARL | RAP PAC | RAPA-EX-01 | |
| Human Longevity Dosing Protocols | Dosing: 2, 4, 5, 6, 8, 10, or 15 mg weekly. Duration: 48 weeks to 1 year (ongoing). Health Status: Healthy adults (ages 50–85). Effects: Improved visceral fat, bone density, and immune markers; enhanced mood, pain, and cognition; fewer severe COVID-19 cases. | Dosing: 5, 10, or 15 mg weekly. Duration: 6 months. Health Status: Healthy adults / older men and women (ages 40–80). Effects: Evaluated anti-aging markers, restored mTOR dynamic range, and potential reduction in chronic inflammation. | Dosing: 5 to 15 mg weekly (specifically 6 mg/week noted). Duration: 12 to 13 weeks. Health Status: Older adults (ages 65–85) with age-related conditions / sedentary. Effects: Monitored for safety, muscle mass maintenance, cardiovascular endurance, and integumentary/skin effects. |
| Dosing Regimen (mg/week) | 2, 4, 5, 6, 8, 10, or 15 mg weekly (commercial and compounded) | 5, 10, or 15 mg weekly | 5 mg to 15 mg weekly (specifically 6 mg/week) |
| Duration of Intervention | 48 weeks to 1 year; noted as ongoing longitudinal study | 6 months (24 weeks) or 6 weeks | 12 to 13 weeks |
| Participant Health Status | Healthy adults / normative aging individuals (ages 50–85) | Healthy adults / older men and women (ages 40–80) | Older adults (ages 65–85) with age-related conditions; sedentary |
| Physiological Systems and Effects | Improved visceral fat, bone density, and immune markers; enhancement in mood, pain, and cognition; reduced severity of COVID-19; modest changes in biological aging biomarkers | Restored mTOR dynamic range; safety (DLTs) and pharmacokinetics; evaluation of glucose metabolism, insulin sensitivity, and chronic inflammation | Maintained muscle mass (strength/chair-stand/handgrip); cardiovascular endurance (6-min walk); monitored for skin side effects (mouth sores) and DNA methylation |
| General Comparison (Inferred) | Low-dose intermittent strategy; well tolerated over 1 year | Geroprotector trial evaluating safety and physiological markers | Specifically monitored for safety and muscle/integumentary system maintenance |
| Primary Objective | Visceral fat and aging biomarkers | Safety and PK/PD in healthy adults | Muscle strength and endurance |
Timing with meals, fasting windows, and training days
For optimal results, users often take rapamycin with a meal containing fats to increase bioavailability, or with grapefruit juice (under medical supervision) to inhibit CYP3A4 and boost blood levels [3]. Dosing is ideally timed on rest days or at least 24-48 hours away from heavy resistance training to minimize the blunting of muscle growth signals [23] [25].
Timing with fasting windows can be strategic. Some users dose at the start of a 24-hour fast to create a “double hit” of autophagy induction [11] [1]. Conversely, because rapamycin is highly lipophilic, its residence in adipose (fat) tissue is prolonged, meaning its metabolic effects can last longer than the drug’s 64-hour half-life would suggest [5] [10] [23].
Safety and Interactions
Rapamycin side effects and drug interactions
Common side effects of rapamycin include mucosal (mouth) ulcers, impaired wound healing, and dyslipidemia [10] [11]. Significant drug-drug interactions occur with CYP3A inhibitors, such as cannabidiol (CBD) and grapefruit juice, which can dangerously increase blood levels and toxicity risk [11] [23].
While low-dose intermittent protocols are generally well-tolerated, they are not without risk [20]. Bryan Johnson followed an elaborate supplement stack. This regimen included rapamycin and metformin. He eventually discontinued these specific treatments. Johnson reported side effects like high susceptibility to infection. He also experienced impaired healing [11].
| Interaction Category | Examples | Effect on Rapamycin |
|---|---|---|
| CYP3A Inhibitors | Grapefruit Juice, CBD, Ketoconazole | Increases toxicity risk |
| CYP3A Inducers | St. John’s Wort, Carbamazepine, Rifampicin | Decreases efficacy |
| P-gp Inhibitors | Cannabinoids, Ciclosporin | Altered absorption |
mTORC1 vs mTORC2 and safety considerations
The “Golden Rule” of rapamycin safety is to selectively inhibit mTORC1 while preserving mTORC2 [7] [2]. While mTORC1 inhibition drives geroprotection, off-target inhibition of mTORC2 is responsible for the deleterious effects on metabolic health, immune function, and survival in male mice [5] [9].
mTORC1 is acutely sensitive to rapamycin, whereas mTORC2 is only inhibited after prolonged exposure [5] [27]. This is why intermittent schedules are safer than daily ones; they give mTORC2 time to “breathe” [2]. Researchers are also developing next-generation rapalogs, like DL001, which are 40x more selective for mTORC1 and do not impair glucose homeostasis in animal models [7].
Who should avoid combination strategies?
Individuals with active infections, compromised wound healing, or a history of malignancies (within 5 years) should avoid rapamycin stacks [11]. Additionally, those with severe congestive heart failure, chronic kidney disease (eGFR < 30), or type 1 diabetes are typically excluded from clinical trials due to the risk of exacerbating their condition [23].
Tracking Outcomes
Blood glucose, lipids, and inflammation markers
Tracking success requires monitoring HbA1C for long-term glucose trends and hs-CRP for systemic inflammation [23]. A successful stack should ideally lead to lower hs-CRP levels (indicating reduced “inflamm-aging”) without significantly elevating fasting glucose or triglycerides [21].
Functional markers: strength, recovery, and energy
Functional tracking is often more insightful than blood work alone. Users should track changes in their 30-Second Chair-Stand Test results, handgrip strength, and self-reported stamina or mood [20] [23].
Longevity biomarkers and trial-style monitoring
Advanced users track their progress with epigenetic clocks like TruDiagnostic or PhenoAge scores. These tools model the net effect of specific health interventions. However, users must view these results as suggestive rather than definitive. Recent illnesses or high-stress events can easily influence the data [20] [23].
What Research Suggests
Rapamycin vs metformin in current longevity evidence
A 2025 meta-analysis confirmed that rapamycin, but not metformin, mirrors the lifespan extension of dietary restriction in vertebrates. While metformin remains a vital tool for metabolic health, rapamycin is the more powerful “longevity drug” for healthy, non-diabetic individuals [6] [19].
Rapamycin and NAD+ in 2026 research updates
The latest research confirms the interconnectedness of the SIRT1 and mTOR pathways [13]. Stacking NAD+ with rapamycin is becoming the preferred strategy for preventing cognitive decline and maintaining mitochondrial bioenergetics during the aging process [4] [20] [22].
What remains uncertain about stacking interventions?
The long-term safety of poly-pharmacy in healthy humans remains the greatest unknown [11]. Definitive Phase 3 trial data does not yet confirm how these stacks impact maximal human lifespan. Users must prioritize medical oversight and rigorous monitoring [2] [20].
Conclusion
Combining rapamycin with metformin and NAD+ precursors represents the cutting edge of preventative medicine. By targeting the mTOR/AMPK/Sirtuin triad, users can theoretically slow the biological clock while protecting their metabolic and physical health. However, the success of these stacks depends entirely on personalization, timing, and cautious monitoring.
If you are considering a rapamycin protocol, start with functional baseline tests (grip strength, walking speed) and a full metabolic blood panel. Make sure your dosing frequency is optimized for your activity level and sex.

Yes, but intermittent dosing (once weekly) is recommended to avoid blunting muscle growth signals during the 24-48 hours after training.
No. Recent meta-analyses show rapamycin has a much stronger effect on lifespan extension in vertebrates than metformin.
Chronic daily use can lead to “benevolent” glucose intolerance or insulin resistance by inhibiting mTORC2, but this is usually avoided with intermittent weekly dosing.
Both NMN and NR are effective at boosting NAD+ levels, with NMN showing particularly strong neuroprotective data in recent rat models.
Initially, every 3-6 months to ensure your dose is within the geroprotective range (5-15 ng/mL) and not reaching immunosuppressive levels.
Resource links
Rapamycin Does Not Compromise Exercise‐Induced Muscular Adaptations in Female Mice
Blazing a trail for the clinical use of rapamycin as a geroprotecTOR
Slowing ageing by design: the rise of NAD+ and sirtuin-activating compounds
A new era of longevity science: models of aging, rapamycin trials, biological clocks, & more
A novel rapamycin analog is highly selective for mTORC1 in vivo
Aging, Rapamycin, Metformin, Resveratrol, Longevity Supplements, David Sinclair, Anti-Aging Myths
Rapamycin-induced insulin resistance is mediated by mTORC2 loss and uncoupled from longevity
Rapamycin for longevity: the pros, the cons, and future perspectives
SIRT1 Negatively Regulates the Mammalian Target of Rapamycin
Immunoregulatory Functions of mTOR Inhibition
Gerosuppressant Metformin: less is more
The first human clinical study for NMN has started in Japan
Is Rapamycin a Dietary Restriction Mimetic?
What is the clinical evidence to support off-label rapamycin therapy in healthy adults?
Targeting ageing with rapamycin and its derivatives in humans: a systematic review
Rapamycin Does Not Compromise Exercise‐Induced Muscular Adaptations in Female Mice