Rapamycin Bioavailability: Why Formulation Is the Hidden Variable in Longevity
The pursuit of longevity often leads researchers and self-experimenters to rapamycin, yet many fail to realize that sirolimus bioavailability is not a fixed number—it is a moving target dictated by chemical engineering. While the active molecule remains the same, the vehicle delivering it determines whether you achieve life-extending mTOR inhibition or simply expensive, unabsorbed waste. Choosing between commercial vs. compounded rapamycin requires a deep dive into nanocrystal physics, gastric acid stability, and the “bioavailability gap” recently quantified in real-world human cohorts.
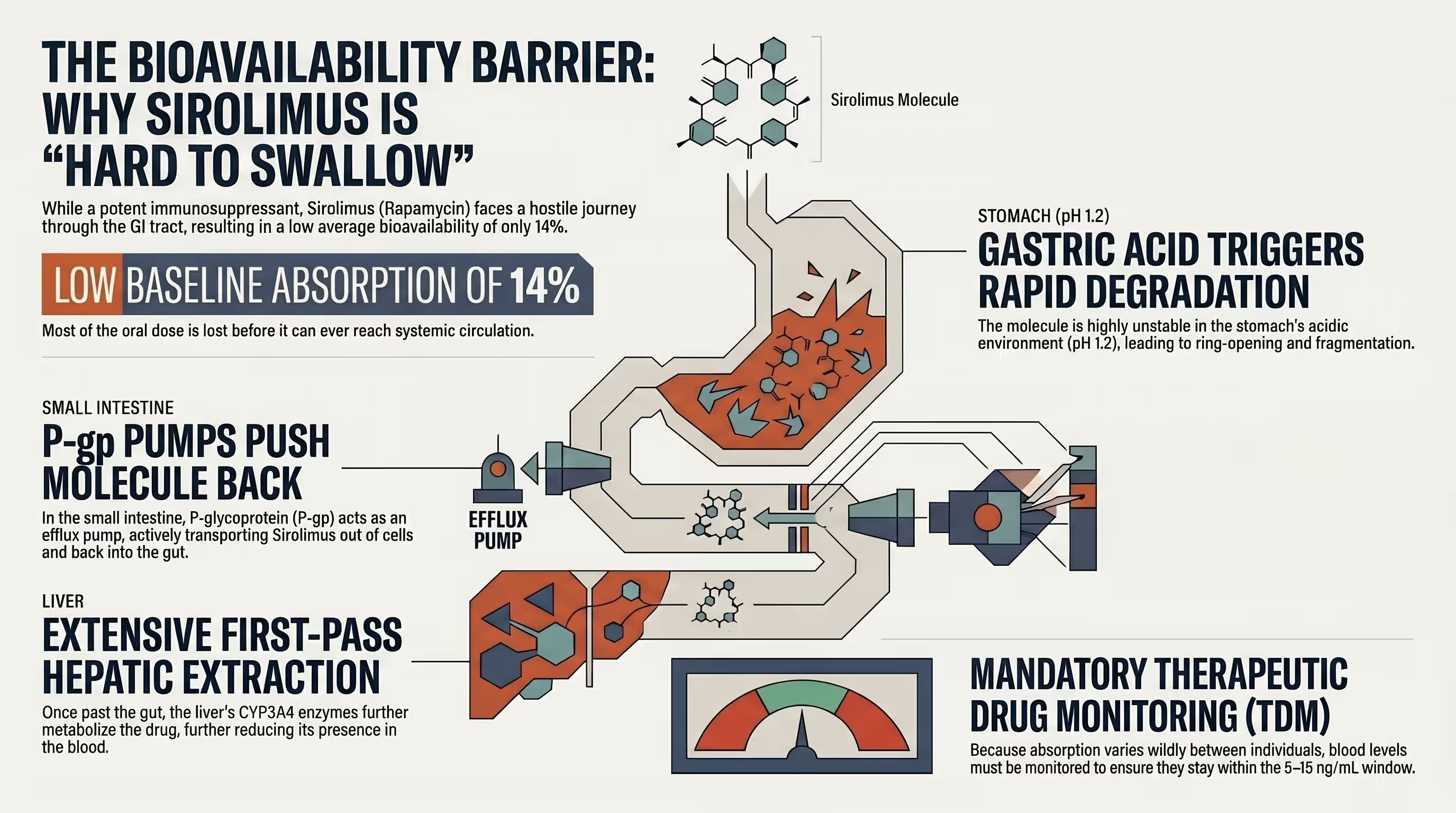
Understanding the Absorption Challenge: Why Rapamycin Is “Hard to Swallow”?
How does the digestive system handle sirolimus absorption?
Sirolimus is a BCS Class II drug, meaning it has high permeability but extremely low aqueous solubility, making it difficult for the body to absorb in its raw form. It is highly lipophilic and subject to aggressive rapamycin first-pass metabolism by enzymes in the gut wall and liver, alongside active rejection by efflux pumps.
The Role of First-Pass Metabolism in Sirolimus Efficacy
The primary obstacle to achieving therapeutic blood levels is the body’s dual-defense mechanism: Cytochrome P450 3A4 (CYP3A4) enzymes and P-glycoprotein (P-gp) transporters. Sirolimus undergoes extensive rapamycin first-pass metabolism in the intestinal mucosa and liver, which drastically reduces the amount of drug that actually reaches systemic circulation. In rat studies, nearly 50% of the parent compound was metabolized within the intestinal mucosa alone before even reaching the liver. This intense metabolic “clearing” is why the average absolute bioavailability of oral sirolimus solution is estimated at a mere 14%. Furthermore, P-gp acts as a biological “bouncer,” actively pumping absorbed sirolimus back into the intestinal lumen, a process that can be inhibited by certain medications or compounds like grapefruit juice to increase exposure.
Lipophilicity and the Barriers to GI Absorption
Rapamycin’s high lipophilicity makes it virtually insoluble in the watery environment of the human digestive tract. This low solubility is the main rate-limiting factor for oral absorption, as the drug must be in a dissolved state to pass through the intestinal epithelial cells. Additionally, sirolimus is chemically unstable in electrolyte solutions, particularly the highly acidic environment of the stomach. In simulated gastric fluid with a pH of 1.2, raw sirolimus experiences rapid GI degradation of sirolimus, often breaking down via ring-opening or fragmentation within minutes. Without a sophisticated delivery system (an engineered enteric coating) to shield the molecule from gastric acid and enhance its solubility, “crude” rapamycin risks being destroyed before it ever reaches the “absorption window” in the small intestine. “Enteric coating is an art and it should be performed by experienced person otherwise different problems may occur (twinning, peeling and frosting, orange peel etc.)”.
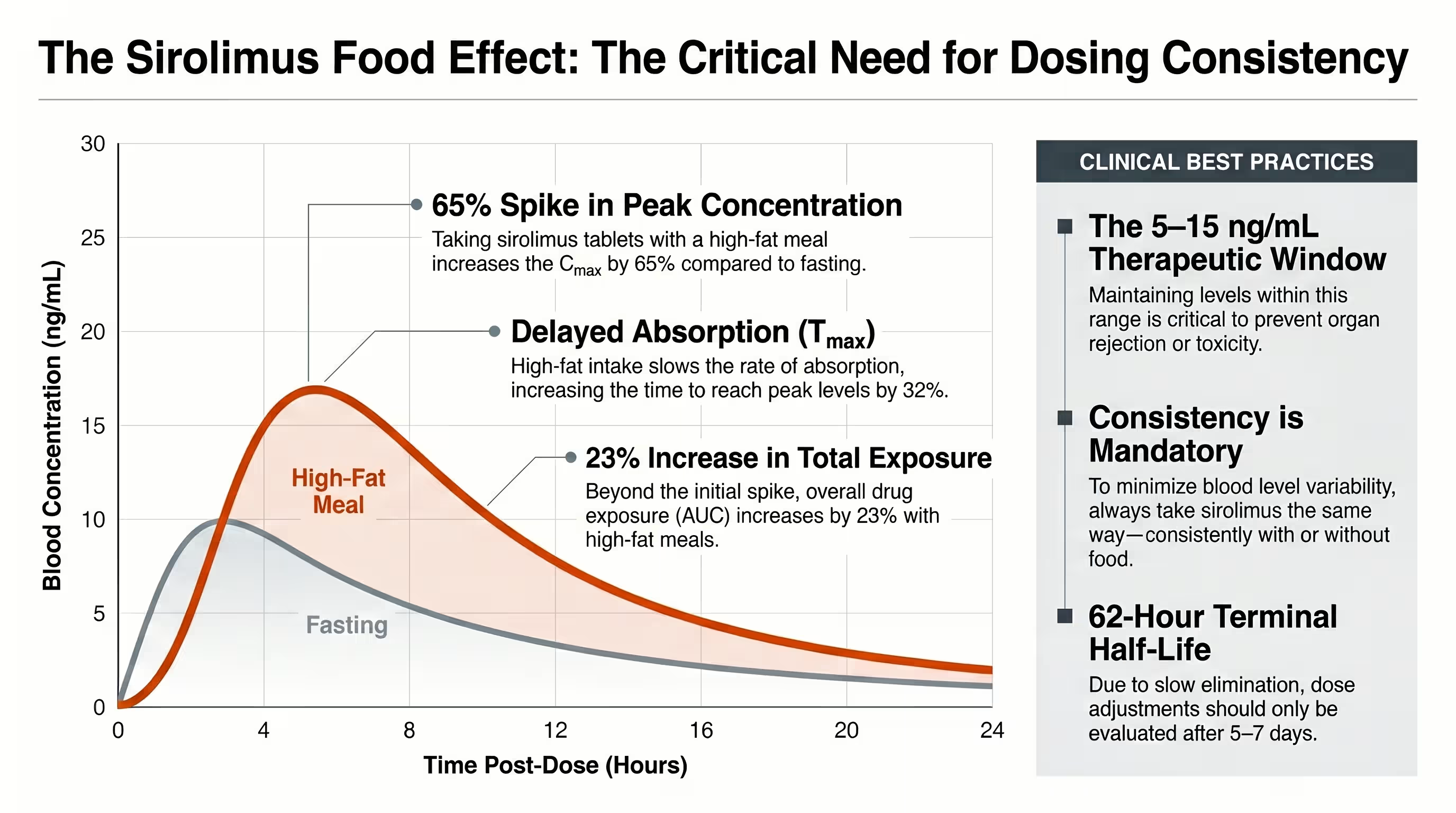
The Impact of High-Fat Meals on Commercial Rapamycin Absorption
Food is a powerful modulator of rapamycin’s pharmacokinetics. Consuming commercial sirolimus with a high-fat meal produces a “food effect” that significantly alters absorption rates. A high-fat breakfast can increase the Cmax by up to 65% and the total AUC by roughly 23% to 35%. While this increase might seem beneficial, it also introduces significant variability into your blood levels. To avoid these fluctuations and maintain stable mTOR inhibition, clinical guidelines recommend taking rapamycin consistently—either always with food or always on an empty stomach.

Compounded Rapamycin: Benefits, Risks, and Variable Bioavailability
Compounded rapamycin offers dosing flexibility and cost savings but often suffers from a significant “bioavailability gap,” with some studies showing it is only 31.03% as bioavailable as commercial versions. This discrepancy is largely due to the use of rapamycin crude powder and the lack of standardized nono particle technologies or high-quality enteric coatings.
The Bioavailability Gap: Why Compounded May Require Higher Doses
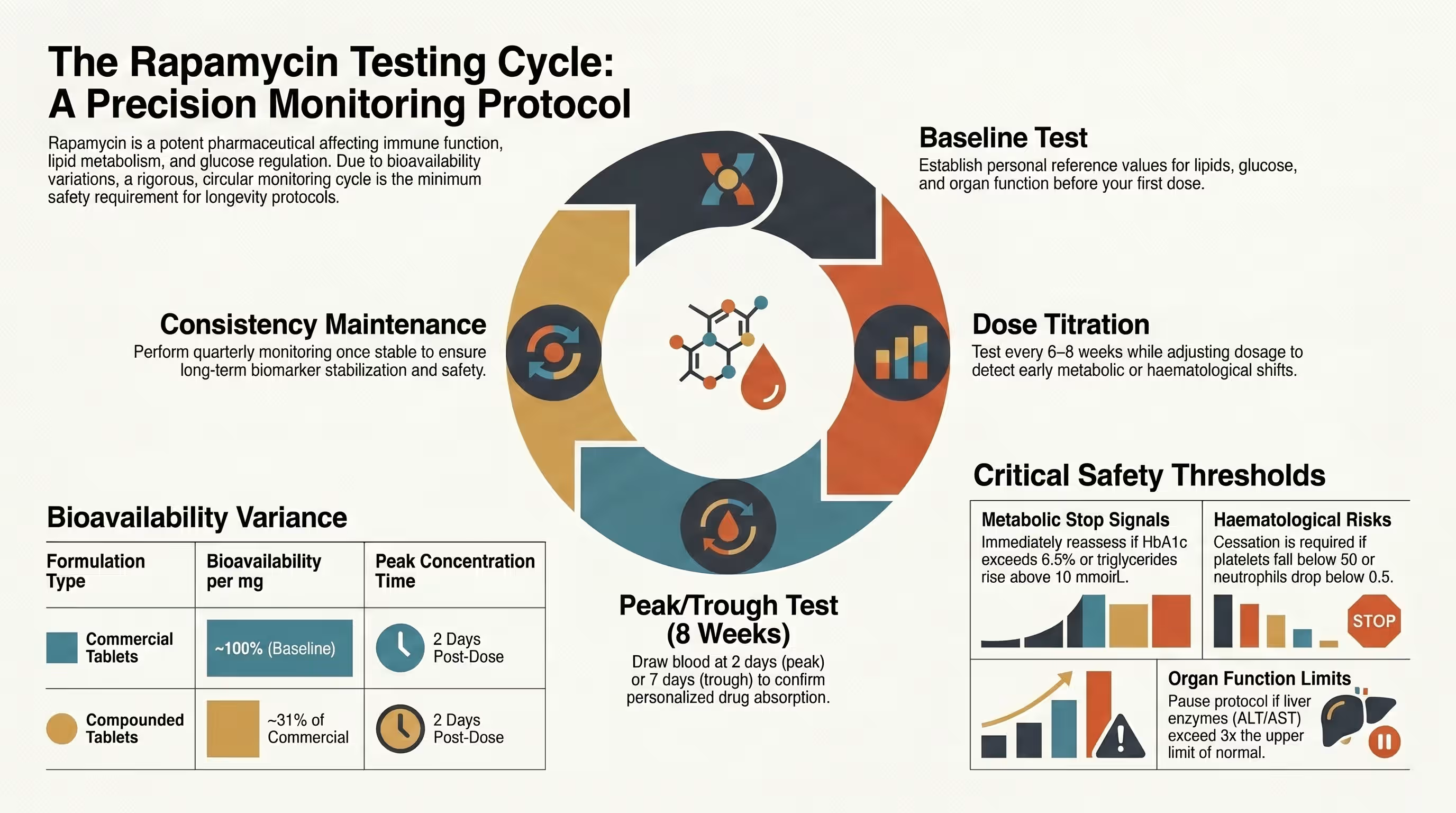
The most striking finding for longevity enthusiasts is the quantified “bioavailability gap.” A large-scale analysis of 316 real-world users revealed that compounded rapamycin bioavailability was significantly lower than commercial generics. Specifically, the estimated blood level for compounded was 0.27 ng/mL per 1 mg dose, whereas commercial versions achieved 0.87 ng/mL per 1 mg dose. This means a user would theoretically need to take three times as much compounded rapamycin to achieve the same blood concentration as the commercial generic. While both formulations show a linear dose-to-blood relationship, the “slope” for commercial rapamycin is significantly steeper, meaning it elicits a much stronger response as the dose increases.
pH-Sensitive Enteric Coating: Protecting Rapamycin from Gastric Acid
Because sirolimus is highly sensitive to the acidic environment of the stomach, the quality of the pH-sensitive enteric coating is a critical variable in compounding. A high-quality enteric coating acts as a barrier that remains insoluble in the low pH of gastric acid but dissolves once it reaches the higher pH (above 5.5) of the small intestine. If a compounded capsule lacks this protection or uses an inferior coating, the drug may degrade before it ever reaches the intestinal “absorption window,” further widening the bioavailability gap. Recent research into amorphous solid dispersions using Eudragit® E has shown that specialized coatings can inhibit sirolimus degradation in a dose-dependent manner, significantly improving oral absorption compared to simple physical mixtures of the powder.
Side-by-Side Comparison: Commercial vs. Compounded Formulations
| Feature | Commercial (Rapamune/Generics) | Compounded (Pharmacy Capsules) |
|---|---|---|
| Technology | NanoCrystal® (Wet-Milled) | Mostly Crude Powder |
| Bioavailability | High (Reference Standard) | Low (~31% of Commercial) |
| Consistency | High (FDA/EMA Regulated) | Variable (Pharmacy-Dependent) |
| Absorption Speed | Tmax ~1-2 hours | Tmax potentially 2 days |
| Gastric Protection | Standard Enteric Coating | Variable Enteric Coating |
| Cost | Higher per mg | Lower per mg |
Case Study: 24-Hour Blood Level Differences in Real-World Cohorts
A 2025 study provided the first foundational look at how these formulations perform in healthy, normative aging individuals rather than transplant patients. Measuring 24-hour blood rapamycin levels, researchers found that while individuals taking the same dose varied substantially in their specific blood levels, the overall trend remained consistent: commercial formulations produced significantly higher peaks. Interestingly, in real-world longevity users, blood levels often didn’t peak until 2 days post-administration, suggesting that the Tmax rapamycin timing for low-dose weekly protocols might be slower than the 1-2 hour peak seen in clinical transplant studies. Despite the lower bioavailability of compounded forms, repeat tests in the same individuals over 6-18 months showed that blood levels eventually stabilized, suggesting that consistency in the brand and pharmacy you use is more important than the formulation itself.
Clinical Implications: How to Optimize Your Rapamycin Protocol
The only way to navigate the variability of sirolimus is through regular rapamycin blood level testing to identify your personal optimized dose. Because individuals can have up to an eight-fold difference in exposure for the same dose, peak and trough testing is the “gold standard” for optimizing a longevity protocol.
The Necessity of Peak and Trough Blood Level Testing
If you are using rapamycin for longevity, blood tests are a minimum safety and efficacy requirement. A “Peak” test (usually 1-2 hours or up to 2 days post-dose in some longevity cohorts) confirms that the drug is actually being absorbed and reaching a level high enough to inhibit mTOR. A “Trough” test (taken immediately before your next scheduled dose) ensures that the drug is clearing your system and not building up to toxic, immunosuppressive levels. Monitoring trough levels is especially critical for those with mild hepatic impairment, as their bodies may clear the drug 33% more slowly, increasing the risk of unintended side effects.
Why Consistency in Formulation Matters for Long-Term mTOR Inhibition
The key to a successful longevity journey is minimizing “hidden variables.” Because generic vs compounded bioavailability varies so wildly, switching between formulations can disrupt your steady-state blood levels. If you must switch, clinical guidelines recommend re-testing your trough concentrations 1 to 2 weeks after the change to confirm you are still within your target range. Consistency extends to your lifestyle as well—taking your dose with the same type of meal at the same time each week is the most reliable strategy for achieving predictable, long-term mTOR inhibition.
Conclusion: Choosing the Right Vehicle for Your Longevity Journey
The real-world data proves that both commercial and compounded rapamycin are bioavailable and can be used effectively. However, the “hidden variable” of formulation means that a 6 mg dose of one might be functionally equivalent to 18 mg of another. By prioritizing rapamycin blood level testing, maintaining strict consistency in your chosen formulation, and understanding the science of nanocrystals and enteric coatings, you can turn sirolimus from a “hard to swallow” challenge into a precisely calibrated tool for healthy aging.

No. Bioavailability has not been determined for tablets that are crushed, chewed, or split, and it is not recommended. Crushing the tablet destroys the specialized coating and nanocrystal structure, likely leading to rapid degradation in gastric acid.
Yes. Grapefruit juice inhibits the CYP3A4 enzyme and P-gp transporter in the gut, which can increase sirolimus exposure by up to 350%. However, this effect is highly unpredictable and can lead to dangerously high blood levels.
Compounded versions often use crude powder, which is found to be about 31% as bioavailable as commercial tablets. You may simply require a higher dose or a switch to a formulation with better enteric protection.
Taking rapamycin with a high-fat meal increases absorption (AUC) by about 23-35%. The most important factor is consistency—always take it with the same type of meal to avoid fluctuating blood levels.
Experts suggest testing at baseline, every 6-8 weeks during your initial dose titration, and then every 3 months once you have achieved a stable, target trough level.
Rapashop offers high quality medical grade Rapamycin tablets, enteric coated to pass through stomach acid for deserved bioavailability.
Resource links
Exposure-response relationships and drug interactions of sirolimus
Sirolimus, PRODUCT MONOGRAPH INCLUDING PATIENT MEDICATION INFORMATION
Absorption and intestinal metabolism of SDZ-RAD and rapamycin in rats
Population Pharmacokinetics of Sirolimus in Healthy Chinese Subjects
Sirolimus formulation with improved pharmacokinetic properties produced by a continuous flow method
Enteric Coated Drug Delivery System
Lipids-based nanostructured lipid carriers (NLCs) for improved oral bioavailability of sirolimus
Rapamycin Monitoring Blood Tests
Absorption and intestinal metabolism of SDZ-RAD and rapamycin in rats
Pharmacokinetics of sirolimus (rapamycin) in subjects with mild to moderate hepatic impairment