Pulsatile vs. Daily Dosing of Rapamycin: Optimizing the Side Effect Profile
Your body’s metabolism is like a high-performance engine. Over time, it builds up cellular waste or “junk”. For decades, researchers sought a biological switch to trigger autophagy. This is a vital self-cleaning mode for cells. Rapamycin is the most promising switch discovered so far. It was originally found in the soil of Easter Island. The biggest question for longevity researchers is how to dose it. They must choose between pulsatile and daily schedules. The goal is to maximize healthspan. However, we must avoid triggering chronic metabolic “stalling.”
Understanding the Dosing Dilemma: Longevity vs. Transplantation
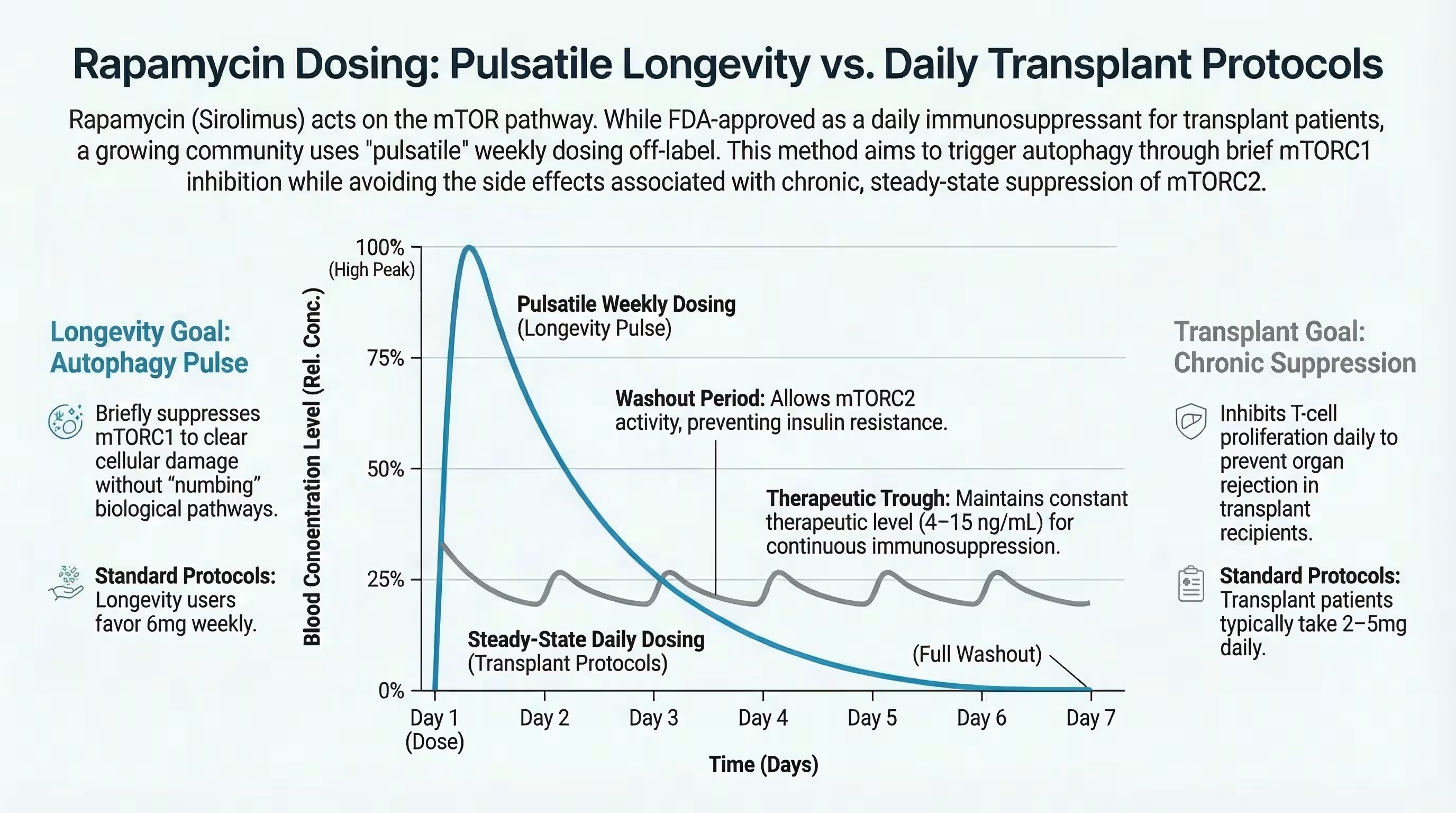
For decades, the clinical use of sirolimus (generic rapamycin) was defined by its role as a daily immunosuppressant used to prevent organ rejection in transplant recipients. In this high-dose context, the goal is constant, deep suppression of the immune system to protect a new organ. However, the longevity community has pivoted toward a “pulsatile” approach to harness the drug’s “geroprotective” benefits while avoiding the toxicity of chronic use. Rapamycin dosing for healthy aging typically involves using a fraction of the transplant dose, administered only once per week or even bi-weekly. This shift is based on the discovery that the benefits for healthspan and lifespan are primarily driven by temporary “pulses” of mTOR inhibition rather than the constant blockade required for transplantation.
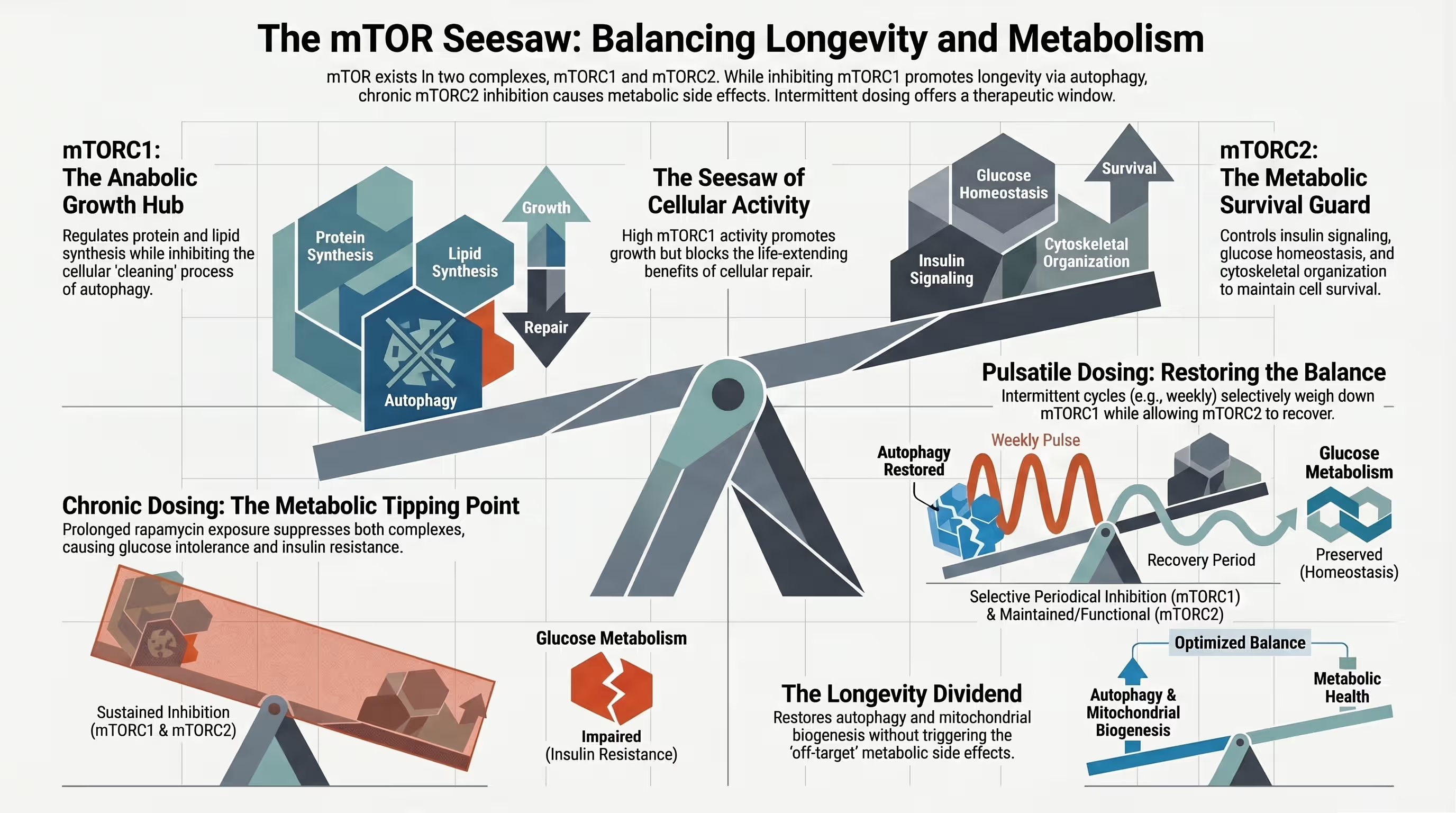
The Biological Switch: mTORC1 vs. mTORC2
The dosing dilemma is explained by a biological reality: the mTORC1 vs mTORC2 inhibition dosing debate. mTORC1 is the primary target for anti-aging; it controls protein synthesis and cellular growth, and its overactivity is a hallmark of aging. While rapamycin is a potent and selective inhibitor of mTORC1, prolonged or daily exposure eventually inhibits mTORC2 as well. This “off-target” suppression of mTORC2 is a fundamental cause of the most severe complications associated with the drug. Users can choose a pulsatile schedule to selectively inhibit mTORC1. This allows for weekly rather than daily rapamycin dosing to trigger autophagy. This method also provides a washout period. Such a break ensures that mTORC2 remains functional.
Side Effect Profile: Daily Dosing (Transplant Protocol)
- Immunosuppression and Infection Risk: Chronic daily dosing keeps rapamycin levels high, which can lead to significant metabolic side effects of daily sirolimus and immune suppression. This creates a high risk for viral and fungal infections, such as pneumonia, urinary tract infections, and skin infections.
- Metabolic Dysregulation: Daily inhibition of mTORC2 leads to rapamycin-induced insulin resistance and severe glucose intolerance. Retrospective data shows that sirolimus is independently associated with an increased risk of new-onset diabetes in transplant recipients. Furthermore, daily treatment often causes a sharp rise in triglycerides and LDL cholesterol in as many as 75% of patients.
- Dermatological Issues: Transplant patients frequently suffer from chronic stomatitis (painful mouth ulcers) and acneiform rashes. Additionally, because mTOR is required for tissue repair, daily dosing is associated with impaired wound healing and persistent surgical pain.

Side Effect Profile: Pulsatile Dosing (Longevity Protocol)
The “Pulse” Advantage: Allowing mTOR Recovery
The primary advantage of pulsatile dosing is that it provides a critical window for cellular recovery. Because the half-life of rapamycin is approximately 60 to 80 hours, a weekly dose allows blood levels to drop significantly by the end of the week. This “trough” period is essential for mTORC2 reassembly, which protects insulin sensitivity and prevents the “diabetes-like syndrome” seen in daily users. Recent human data, including the PEARL trial rapamycin results, confirm a key finding. These intermittent “longevity doses” do not act as broad immunosuppressants. Furthermore, healthy aging adults generally tolerate them well.
Common Mild Effects in Pulsatile Users
- Transient Aphthous Ulcers: Often referred to as “Rapa-sores,” these small mouth ulcers are the most common intermittent rapamycin side effects even in pulsatile protocols. A survey of 333 adults analyzed the occurrence of mouth ulcers with intermittent rapamycin dosing. These ulcers occurred in 14.7% of users. In contrast, only 4.7% of non-users reported having them. They are typically shallow, painful, and appear on the non-keratinized mucosa.
- Gastrointestinal Sensitivity: The PEARL trial rapamycin results show that GI symptoms were reported. These included nausea or loose stools. Rapamycin users experienced these slightly more often than the placebo group. These effects are usually acute. They typically resolve without needing to stop the medication.
- Sleep and Energy Fluctuations: While some users report acute fatigue shortly after a dose, long-term survey data suggests that 34.8% of users feel “happier” and 38.7% report having more energy.
Comparative Analysis: Clinical Data and Trials
| Side Effect | Daily Dosing (High Dose) | Pulsatile Dosing (Low Dose) |
|---|---|---|
| Diabetes Risk | High (Up to 32% new-onset) | Very Low / Neutral |
| Mouth Ulcers | Very High (Up to 60-70%) | Moderate (Lower incidence) |
| Infection Risk | Significant (Immunosuppressive) | Low (May improve immune response) |
| Lipid Profile | High incidence of hyperlipidemia | Mild, transient increases |
| Target Trough | >5 ng/mL | <3 ng/mL |
Optimizing Your Protocol: Monitoring and Safety
Essential Biomarkers for Pulsatile Users
Safe navigation of a longevity protocol requires regular blood work to monitor low-dose intermittent rapamycin safety. Users should track a fasting lipid panel, glucose, and HbA1c every 3 to 6 months to detect any early signals of rapamycin-induced insulin resistance daily vs pulse. Measuring sirolimus trough levels for longevity—taken just before the next weekly dose—helps confirm that the drug is clearing the system properly and staying below the safety threshold.
The Role of Pharmacokinetics: Half-life and Washout Periods
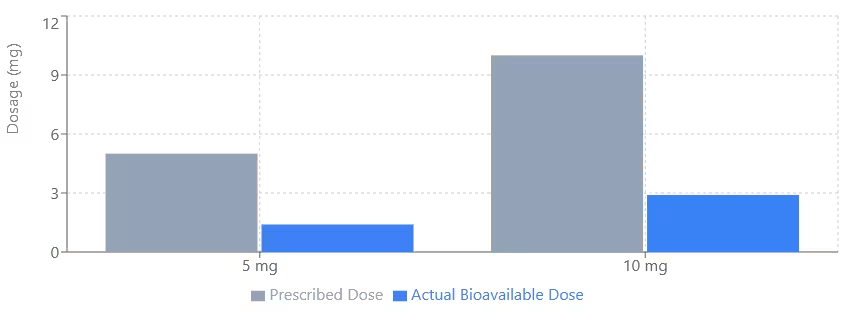
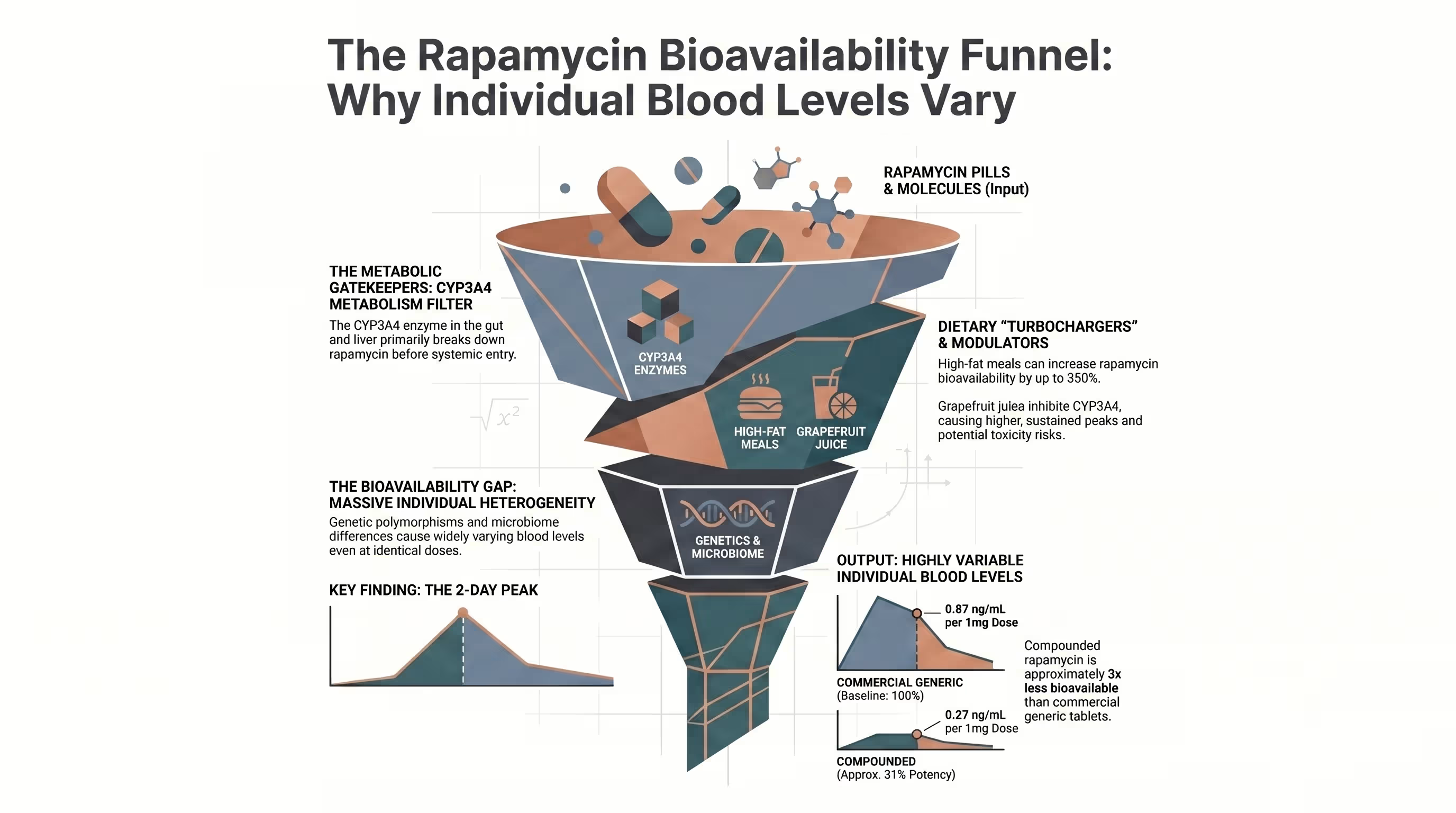
Understanding the pharmacokinetics of rapamycin is critical because “one dose does not fit all”. Bioavailability can vary up to 3.5-fold between compounded rapamycin relative to generic. Factors like high-fat meals or the activity of the CYP3A4 enzyme in the liver significantly change how much drug enters the bloodstream (bioavailability).
Conclusion: The Shift Toward Intermittent Precision
The weight of evidence from both animal models and human trials like PEARL suggests that rapamycin dosing for healthy aging is moving away from the blunt force of daily protocols toward intermittent precision. By using a weekly “pulse,” you can effectively inhibit mTORC1 to stimulate autophagy while preventing the chronic destruction of mTORC2 that leads to insulin resistance. While mild side effects like “Rapa-sores” and GI sensitivity remain a reality for some, they are typically manageable with proper monitoring and personalized dose tailoring. For those pursuing longevity, the goal is clear: utilize the pulse to “add life to years” without sacrificing the metabolic engine that keeps us healthy.

In the PEARL trial, there was no massive overall weight loss across all groups. However, some participants showed improvements in visceral adipose tissue (VAT) and females showed a significant increase in lean tissue mass, suggesting a benefit for body composition rather than simple “pounds lost”.
The most effective treatment identified in clinical literature is a steroid-based mouthwash, such as dexamethasone. Maintaining excellent oral hygiene and avoiding acidic foods during a flare-up can also help manage the pain.
While rapamycin is an immunosuppressant at high, daily doses, studies in the elderly have actually shown that low-dose mTOR inhibitors can improve the immune response to vaccines and reduce the frequency of infections by rejuvenating T-cells.
Chronic daily rapamycin is known to cause glucose intolerance and can worsen diabetes. While pulsatile dosing is designed to mitigate this risk, anyone with poorly controlled diabetes should avoid rapamycin until their baseline is stabilized and they are under strict medical supervision.
Grapefruit juice inhibits the CYP3A4 enzyme, which can increase rapamycin blood levels by 3-fold to 5-fold. While some biohackers use this to save money, it makes dosing highly unpredictable and is generally not recommended for longevity protocols.
Resource links
Rapamycin for longevity: the pros, the cons, and future perspectives
Inhibition of the Mechanistic Target of Rapamycin (mTOR)-Rapamycin and Beyond
mTOR Inhibitor Therapy and Metabolic Consequences: Where Do We Stand?
Recent insights into the pathophysiology of mTOR pathway dysregulation
Rapamycin in aging and disease: maximizing efficacy while minimizing side effects
Influence of rapamycin on safety and healthspan metrics after one year: PEARL trial results
Intermittent Administration of Rapamycin Extends the Life Span of Female C57BL/6J Mice
Targeting mTOR with rapamycin: One dose does not fit all
Impact of rapamycin on longevity: updated insights
Safety and efficacy of rapamycin on healthspan metrics after one year: PEARL Trial Results
Evaluation of off-label rapamycin use to promote healthspan in 333 adults
Influence of rapamycin on safety and healthspan metrics after one year: PEARL trial results