Starting Rapamycin: The 3-6mg Protocol and What to Expect

Optimizing a Rapamycin Protocol for healthy aging is rapidly shifting from speculative biohacking to a data-driven clinical science. As more normative aging individuals look to geroprotective compounds, physicians and researchers are moving beyond the theoretical mechanisms of mTOR inhibition to focus on real-world pharmacokinetics, bioavailability, and precise dosing regimens. You are likely already aware that rapamycin is a potent immunosuppressant traditionally used in organ transplantation, but its off-label application for longevity requires a fundamentally different approach to avoid toxicity.
For those focusing on healthspan extension, the most widely adopted and researched regimen is the intermittent 3-5mg protocol. Below, we dive directly into the clinical data, advanced dosing mechanics, user sentiment, and safety monitoring required when starting rapamycin.
[Developer Note: Suggest Image 1 here – A high-quality, clinical photograph of a physician reviewing a pharmacokinetic blood concentration chart on a tablet. Alt text: “Clinical evaluation of rapamycin blood level pharmacokinetics and bioavailability over a 7-day dosing period.”]
What is the Standard Longevity Dose for Rapamycin?
The standard off-label longevity dose for rapamycin is typically 3 to 6 mg taken orally once a week. This intermittent, pulsatile schedule aims to selectively inhibit the mTORC1 pathway while allowing a washout period that minimizes the suppression of mTORC2, avoiding the metabolic and immunosuppressive side effects associated with daily dosing.
While clinical trials in humans are still working to establish a definitive dose-response curve, real-world data and expert consensus heavily favor intermittent, weekly dosing. In longevity medicine practice, starting doses usually follow a “start low, go slow” methodology, beginning at 2 to 3 mg per week and cautiously titrating up to 5 or 6 mg.
Why Choose 3-6mg for Longevity?
This dose targets mTOR inhibition for autophagy and lifespan benefits seen in animals, translated to humans via trials showing biomarker shifts without major safety flags.
Animal data first spotlighted rapamycin: mice lived 20-60% longer on intermittent low doses, reducing aging hallmarks like inflammation. Human translation lags, but PEARL‘s one-year trial on healthy adults found low weekly doses well-tolerated, with modest aging biomarker improvements—no metabolic or organ damage versus placebo.
Peter Attia calls it “promising” but cautions human data is early; no FDA nod for longevity yet. Matt Kaeberlein, after self-experimenting, noted 90% joint pain reduction in 2.5 months on weekly doses.
Rapashop‘s generics (Rapacan, Siromus) match Pfizer Rapamune bioavailability, ideal for precise 3-6mg dosing.

Formulation Matters: Commercial vs. Compounded Bioavailability
A critical and frequently overlooked factor in any rapamycin protocol is the profound difference in bioavailability between generic commercial tablets and compounded capsules. Because rapamycin is a highly lipophilic (fat-soluble) molecule, its absorption in the human gut is notoriously poor without specialized delivery systems.
Recent 2025 clinical data analyzing real-world longevity cohorts revealed that compounded rapamycin is significantly less bioavailable than commercial generic formulations (like Biocon, or Zydus). Specifically, blood rapamycin levels from compounded formulations yield only about 31% of the concentration per milligram compared to commercial tablets. If you are targeting a 5mg compounded capsule, your systemic exposure may actually be equivalent to taking roughly 1.5mg of a commercial tablet.
Furthermore, longitudinal tracking shows that the rapamycin half life and systemic clearance dictate that blood levels peak exactly 2 days post-dose, gradually declining over the remainder of the week. This pharmacokinetic curve provides the foundational logic for the 7-day intermittent dosing interval.
What Does Rapamycin Inhibit and How Does It Extend Healthspan?
Rapamycin primarily inhibits the mechanistic target of rapamycin complex 1 (mTORC1), a crucial cellular nutrient and growth sensor. By acutely blocking mTORC1, rapamycin mimics a state of nutrient scarcity, which triggers cellular autophagy—the body’s internal recycling process that clears out damaged proteins, dysfunctional mitochondria, and senescent cells.
Chronically high mTOR activity is intimately linked to accelerated aging, stem cell exhaustion, and age-related chronic inflammation (“inflammaging”). While daily, high-dose rapamycin administration effectively suppresses the immune system for transplant patients, intermittent low dosing shifts cellular activity from anabolic growth processes toward maintenance and repair.
Recent human trials demonstrate the tangible downstream effects of this mTORC1 inhibition. In the 2024 PEARL (Participatory Evaluation of Aging with Rapamycin for Longevity) trial, healthy adults taking weekly rapamycin demonstrated dose-dependent and sex-specific improvements. Most notably, female participants taking 10mg of compounded rapamycin per week gained an average of 4.5% in lean tissue mass and reported significant reductions in overall pain.
Furthermore, low-dose rapamycin appears to exert an immunomodulatory, rather than immunosuppressive, effect. Clinical trials led by Dr. Joan Mannick demonstrated that healthy older adults given low-dose mTOR inhibitors exhibited a 20% increase in immune titers following influenza vaccination, alongside a reduction in circulating PD-1 positive CD4 and CD8 cells—a marker of a more youthful, resilient immune phenotype.
What Side Effects Occur at 3-6mg?
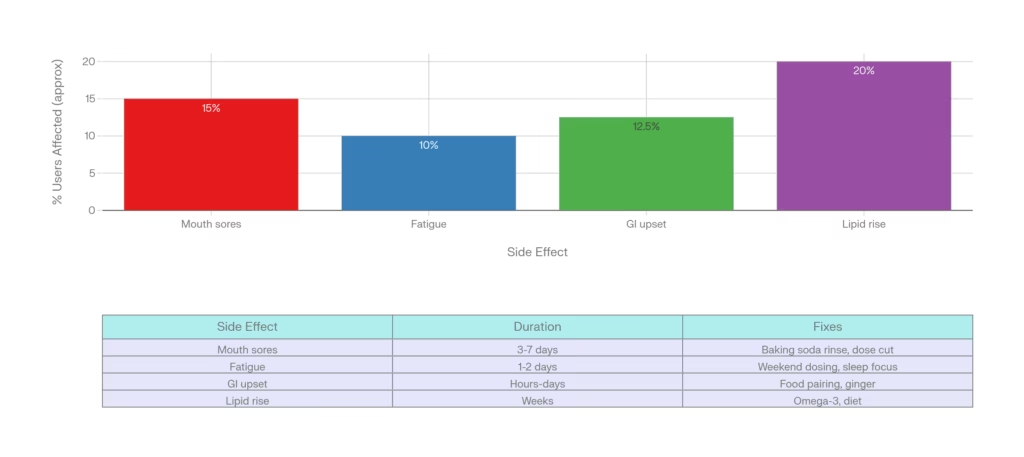
The most frequent side effect of low-dose rapamycin is aphthous stomatitis (mouth sores), which occurs in approximately 15% to 40% of users. Other well-documented side effects include transient hyperlipidemia (elevated LDL and triglycerides) in 5-20% of the users, minor GI (gastrointestinal) upset, and temporary fatigue immediately following the weekly dose.
While survey data of off-label users indicates that intermittent rapamycin is generally well-tolerated, it is a potent prescription drug with real clinical risks. The side effect profile shifts significantly if the drug inhibits mTORC2, which occurs with excessively high doses or overly frequent administration.
- Metabolic Shifts: It is common for users to observe a “lipid bump.” Clinical evaluations, such as the Kraig et al. study, noted significant increases in triglycerides and Hemoglobin A1c (HbA1c) in some subjects. Real-world users frequently track this closely; as one user in the r/LongevityEssentials community noted, they experienced a “small bump in LDL and a pretty noticeable drop in inflammation markers” after starting a 4-6mg weekly protocol.
- Immune Considerations: While low doses enhance specific immune responses, higher continuous exposure carries the traditional risks of immunosuppression, including delayed wound healing and increased susceptibility to bacterial infections.
Low-dose weekly use keeps serious risks low, unlike transplant regimens. PEARL reported no moderate-severe events beyond placebo. Mouth ulcers top lists—rinse with baking soda; acne responds to benzoyl peroxide.
How Does the Body Respond Week 1-4?
Users that take low dose Rapamycin on a weekly schedule would expect subtle shifts: peak blood levels day 2, autophagy boost peaking days 3-5, possible mild fatigue or mouth tingling by day 4-7.
Pharmacokinetics show stable trough levels after consistent weekly 3-5mg, per 2025 study. mTOR dips promote cell cleanup, potentially easing inflammation.frontiersin+1
Week 1 users feel nothing or light tiredness. By week 4, some note clearer skin, steady energy post-initial dip. 26-year-old on 2-6mg saw endurance hit but adapted.
No big metabolic crashes at this dose, unlike high ones. Track subjective energy, sleep.
[Suggested Image: Timeline graphic showing blood levels, autophagy peaks, and side effect windows for week 1 dose. Alt Text: “Rapamycin 3-5mg timeline: blood levels peak day 2, effects through week.”]
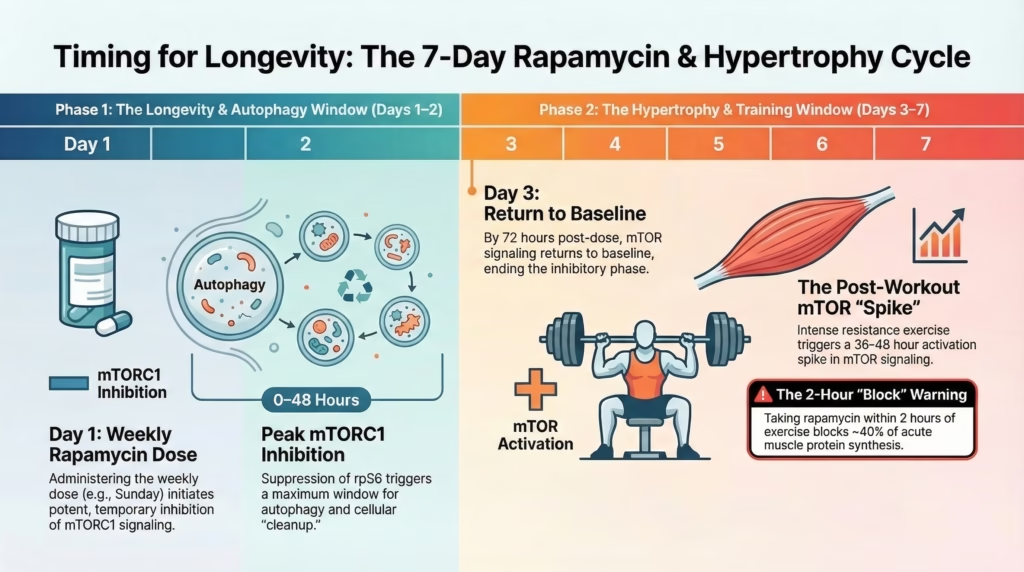
Rapamycin and Exercise: Does It Blunt Muscle Protein Synthesis?
A persistent question regarding the 3-6mg protocol is how it interacts with physical training. Because mTORC1 activation is a required pathway for muscle hypertrophy, there is a theoretical concern that rapamycin might blunt muscle growth. Clinical data presents a mixed picture: one study showed 16mg blunted post-exercise protein synthesis, while another showed no alteration in basal synthesis rates.
Anecdotally, user sentiment from forums like r/Rapamycin highlights a transient drop in athletic performance. A 26-year-old user reported, “Rapamycin will seriously affect your endurance capacity for a day or two afterwards. I simply can’t row and run as hard… Also, there has been a decrease in the ‘pump’ I get”. Consequently, the best day of the week to take rapamycin is usually chosen strategically to align with rest days, allowing users to sleep through initial fatigue and avoid heavy resistance training during peak blood concentration levels.
How to Test Rapamycin Blood Levels and Track Success?
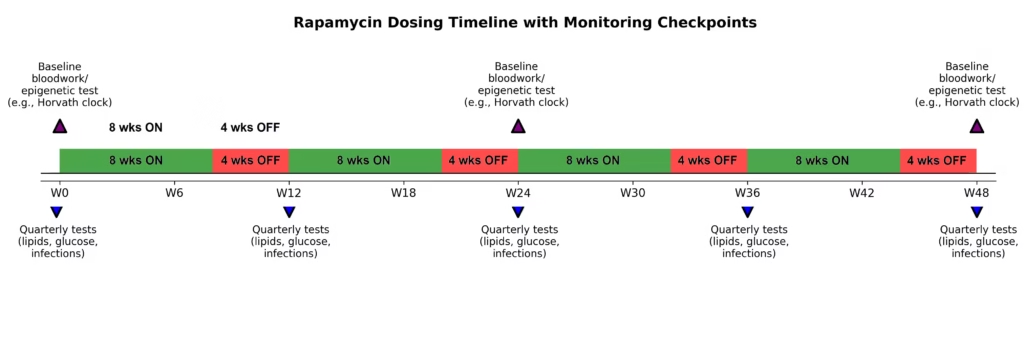
To effectively ensure your protocol is safe and therapeutic, you must undergo routine blood testing, specifically a liquid chromatography/mass spectrometry “Sirolimus assay.” Clinicians recommend testing trough levels (just before your next weekly dose) to ensure clearance, and testing comprehensive metabolic panels every 3-6 months to monitor lipid and glucose shifts.
Given the massive inter-individual variability in absorption, relying solely on standard dosages without objective verification is a flawed strategy. Dietary factors drastically alter absorption; taking your dose with a high-fat meal can increase systemic exposure, while compounds like grapefruit juice inhibit the CYP3A4 enzyme, unpredictably spiking drug levels in the blood.
To track your biological response safely, implement the following testing cadence under physician supervision:
- The Sirolimus Assay: Check your peak (48 hours post-dose) or trough (Day 7, right before your next dose) blood concentration. This confirms you are absorbing the drug without accumulating toxic immunosuppressive levels.
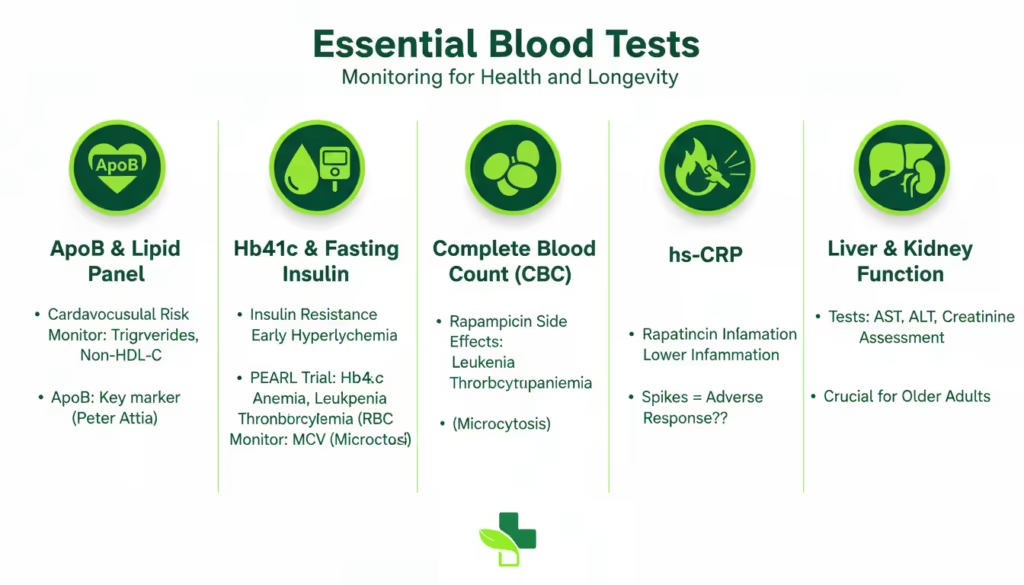
- Advanced Lipid Panels: Monitor ApoB, LDL, HDL, and triglycerides. If hyperlipidemia occurs, your physician may adjust your dose or introduce lipid-lowering interventions.
- Metabolic Markers: Track Fasting Insulin, Fasting Glucose, and HbA1c to detect any mTORC2-induced insulin resistance.
- Complete Blood Count (CBC) & CMP: Monitor white blood cell counts, red blood cell distribution width (RDW), liver enzymes (ALT/AST), and kidney function to ensure baseline physiological safety.
Data Comparison: Commercial vs. Compounded Rapamycin Dosing
| Formulation Type | Common Longevity Dose | Estimated Bioavailability (ng/mL per 1mg) | Primary Clinical Benefit | Potential Drawbacks |
|---|---|---|---|---|
| Commercial Tablets (e.g., Biocon, Pfizer) | 2 mg – 6 mg Weekly | ~0.87 ng/mL | Highly consistent absorption; utilizes nanocrystal technology. | Less dosing flexibility; higher cost in some regions. |
| Compounded Capsules | 5 mg – 15 mg Weekly | ~0.27 ng/mL (approx. 31% of commercial). | Highly customizable titration; easier to combine with other compounds. | Requires much higher raw milligram doses to achieve therapeutic blood levels. |
(Data derived from 2025 retrospective real-world cohort analysis on Sirolimus bioavailability).
Real User Experiences at 3-5mg?
Biohackers report 70-90% tolerate well: better recovery, skin, but 20% note transient workout slumps or sores.
A 2+ year 5mg weekly user (started at 25) dialed back from 10mg, saw anti-aging potential sans major issues. Young user (26): “Endurance down 1-2 days, pump less, but tolerable.”
Longevity clinic patient on Rapashop.net: bloodwork “wilder than expected” after 3 months, positive overall. Kaeberlein: shoulder healed fast.
Some users quit over lipids. Women often fare better. A Reddit user shared his experience as “After 2 years on 5mg weekly, I’m convinced—subtle but real longevity edge.”
Sourcing Quality Rapamycin for 3-5mg?
Opt for lab-tested generics like Rapashop.net.
Indian gens (Biocon Rapacan & Zydus Siromus) shine in community tests for trough levels.
Avoid unverified; test purity.

Conclusion
Transitioning to a 3-5mg rapamycin protocol requires abandoning the mindset of standard nutritional supplementation and adopting the rigor of clinical gerotherapeutics. While the preclinical data showing delayed cellular senescence and extended lifespan across model organisms is overwhelming, human translation remains nuanced.
The clinical evidence supports that an intermittent, weekly dose of commercial rapamycin safely targets the mTORC1 pathway while mitigating severe side effects. However, the occurrence of lipid spikes, temporary fatigue, and mouth sores, coupled with profound variations in individual bioavailability, makes physician-guided blood monitoring non-negotiable.
Before modifying your longevity strategy, consult with a longevity-literate physician. Demand baseline blood panels (including a Sirolimus assay, lipids, and HbA1c) to objectify your starting point. Do not guess your dosage—measure your biochemistry.

Mouth sores or fatigue hit 3-7 days post-dose, fading fast.
Yes, matches trials showing mTOR benefits sans high-dose risks.
Baseline CBC, lipids, metabolic panel essential.
Yes, often better tolerated per PEARL.
Highly rated for generics, worldwide delivery.
Rapamycin tablets are enteric coated to pass gastric acid, and to get metabolized at the intestine.
Resource links
Blazing a trail for the clinical use of rapamycin as a geroprotecTOR
What is the clinical evidence to support off-label rapamycin therapy in healthy adults?
Results of a Crowdfunded One-Year Human Rapamycin Trial
What is the recommended dosing for rapamycin (sirolimus) for longevity?
Longevity, aging and rapamycin
First Results from the PEARL Trial of Rapamycin
Rapamycin Side Effects: Complete Safety Guide
Best Rapamycin Brands, Generics & Compounds
Rapamycin for longevity: the pros, the cons, and future perspectives
REDDIT: Young people(under 30) taking rapamycin, what has your experience been with it?
REDDIT: Anti-aging experiment: I have been taking weekly rapamycin for over 2 years - AMA




