Does Rapamycin Affect mTORC2 and Why Is That Dangerous?
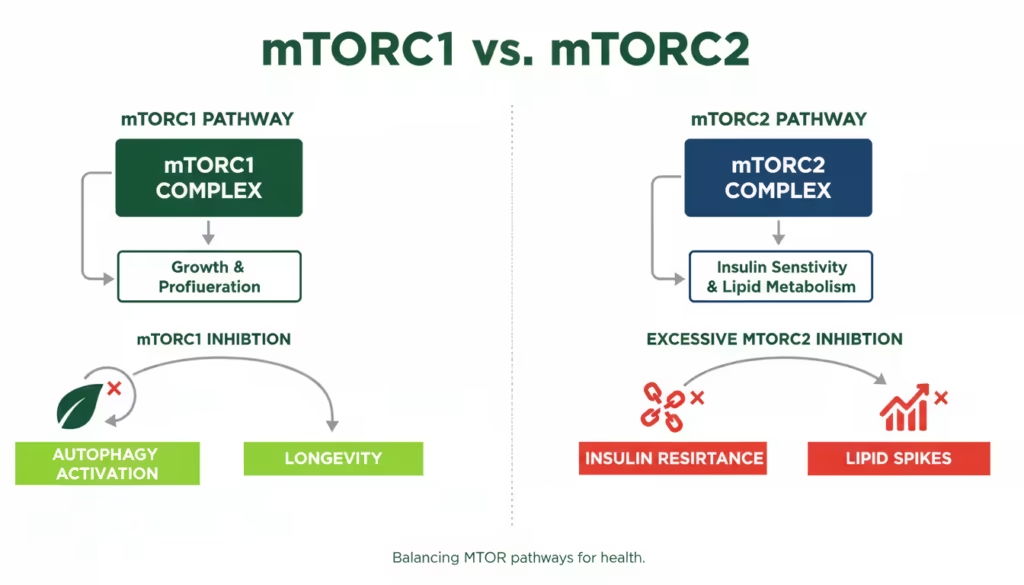
Rapamycin inhibits mTORC1 rapidly but can disrupt mTORC2 with prolonged or high exposure, potentially leading to insulin resistance, immune suppression, and endothelial damage—serious risks for longevity seekers. Intermittent low dosing minimizes mTORC2 impact while preserving benefits like autophagy induction. Experts like Peter Attia and Matt Kaeberlein advocate pulsed protocols to balance these effects.
How Does Rapamycin Inhibit mTORC2?
Rapamycin binds FKBP12 to allosterically inhibit mTORC1 quickly, but chronic exposure sequesters free mTOR, preventing mTORC2 assembly and causing prolonged inhibition after days to weeks. This off-target effect emerges at doses over 2 mg/kg daily in mice or sustained high levels in cells.
mTORC2 regulates Akt signaling, cytoskeletal organization, and cell survival, distinct from mTORC1’s growth control. Studies show rapamycin at 100 nM for 24 hours in human endothelial cells triggers apoptosis and necrosis via mTORC2 loss, worsened by inflammation like TNFα. In vivo, mice on chronic rapamycin develop hyperglycemia and hyperlipidemia tied to mTORC2 disruption.
Intermittent dosing exploits kinetic differences: mTORC1 rebounds faster, avoiding mTORC2 hit. A mouse study with 2 mg/kg every 5 days extended lifespan without glucose issues, unlike daily dosing.
Why Is mTORC2 Inhibition Dangerous?
mTORC2 inhibition by rapamycin risks metabolic syndrome (insulin resistance, dyslipidemia), weakened immunity, and vascular damage, counteracting longevity goals. These stem from impaired Akt phosphorylation, reducing insulin signaling and nitric oxide production.
Human data echoes this: young men on single 6 mg doses saw insulin sensitivity rise via mTORC1 alone, but chronic rodent regimens caused fasting insulin spikes (104 vs 86 pmol/L). Endothelial studies link it to actin stress fibers, reduced motility, and prolonged inflammation—key for atherosclerosis. Gender differences appear: males suffer more longevity hit from partial mTORC2 loss, per Rictor heterozygote mice.
Longevity researchers note mTORC2 as essential for healthspan; its knockout shortens male mouse life. User reports on Reddit align: chronic low daily (1 mg) users note fatigue and insomnia, possibly early mTORC2 signs.
What Do Clinical Studies Show on Rapamycin and mTORC2?
Peer-reviewed trials confirm chronic rapamycin hits mTORC2, causing side effects, but intermittent human pilots (3-6 mg weekly) show mTORC1 benefits with minimal metabolic disruption.
A crowdfunded one-year human trial found weekly rapamycin improved immune markers without major glucose intolerance, unlike transplant daily dosing. Mouse intermittency (every 5 days) preserved respiratory exchange ratio, indicating intact mTORC2, and extended life 18-23%. Recent 2024 reviews stress selectivity: rapalogs aim for mTORC1-only to avoid these pitfalls.
Conflicting data exists—intermittent didn’t fully rescue testicular pathology or heart fibrosis in mice—but reduced overall inflammation vs continuous. No large human longevity RCTs yet, but Dog Aging Project monitors weekly low-dose safety.

Expert Views: Attia and Kaeberlein on mTORC2 Risks
Peter Attia uses 6 mg weekly rapamycin pulsed, emphasizing intermittent avoids mTORC2/insulin issues; Matt Kaeberlein concurs, rating it highly for longevity if dosed right.
Attia continues low-dose for immune boost in elderly context. Kaeberlein highlights the benefits of transient inhibition: weekly hits mTORC1 for autophagy without chronic downsides. In 2025 talks, both praise selectivity via pulsing.
They warn: context matters—transplant daily dosing immunosuppresses via both complexes; longevity uses leverage pharmacokinetics (long half-life sustains mTORC1 hit 3-5 days).
User Experiences with Rapamycin and Side Effects
Forum users report success with intermittent dosing avoiding mTORC2-like issues, but daily users flag fatigue and mouth sores.
On Reddit’s r/Rapamycin, one switched from 1 mg daily (fatigue, insomnia) to weekly, resolving symptoms. Another at 2-5 mg weekly noted headaches but persisted, tying to lipids/insulin checks. Rapamycin.news users praise Rapashop.net for being affordable, and offering good customer support.
A survey of off-label users found 6 mg weekly most common, with ulcers (resolving months) and mild fatigue anecdotal; higher/chronic raised lipids. These echo studies: pulsing aligns with safety.
Intermittent Dosing: Minimizing mTORC2 Danger
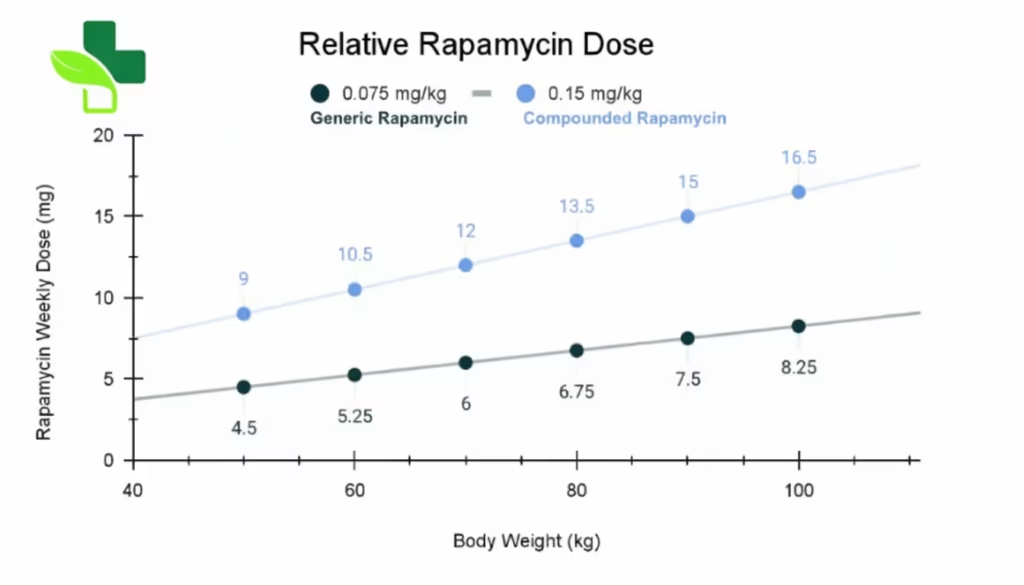
Dose rapamycin 3-10 mg weekly (e.g., 6 mg) to target mTORC1 selectively, as half-life sustains inhibition 3-7 days without mTORC2 accrual.
- Start low: 3-5 mg/week, monitor lipids/glucose 4 weeks in.
- Pulse: Single dose, skip 6 days; repeat.
- Track: Bloodwork for insulin, HbA1c, CRP.
- Sources: Reputable like Rapashop.net
This mirrors mouse success: every 5 days extended life sans metabolic hits. Humans show similar pharmacokinetics.
| Dosing Regimen | mTORC2 Risk | Key Benefits | Common Sides |
|---|---|---|---|
| Daily (1-5 mg) | High | Strong autophagy | Fatigue, insulin resistance |
| Weekly (3-10 mg) | Low | Lifespan extension, immunity | Mild mouth sores reddit |
| Every 2 weeks | Minimal | Maintenance | Rare |

Conclusion
Rapamycin’s mTORC2 inhibition poses real dangers like metabolic and vascular harm from chronic use, but intermittent low dosing sidesteps this for safe longevity pursuit. Key: prioritize pulsed protocols per experts and studies.
Explore pharmaceutical-grade options at Rapashop.net—trusted by users for purity and ease. Consult your physician before starting.

Yes, kinetics favor mTORC1 selectivity; studies show no glucose disruption.pmc.ncbi.nlm.nih+1
Rising fasting insulin, fatigue, lipid changes—monitor via bloodwork.
Promising in pilots, but off-label; intermittent minimizes risks.
Rapashop offers an expedited 10-day delivery, free with every order.